 Updated July 1, 2023
Updated July 1, 2023
List of questions
Updated July 1, 2023
List of questions
| This color text ... | Quotes from the internet |
| This color text ... | My comments |
| Underlined text ... | My emphasis added |
Youtubes
TL;DR
Vaccines
How do you know who to believe?
I'm tired of COVID-19.
Is the juice worth the squeeze?
How bad is it, really?
What's the risk?
How do we kill it?
How to be wrong
Just the facts
Church people
https://www.youtube.com/playlist?list=PLEb9Wh_GlgF5VUpBmG1G_4WkgoGRdWT6u
COVID is high risk.
Vaccines are low risk.
Masks are no-risk for adults.
Act like you have COVID. (YouTube)
Protecting vulnerable individuals and populations
You will someday be old or sick.
How to discuss controversial topics
2020 & 2021 US deaths compared to past years
Unvaccinated vs vaccinated COVID deaths
Post-vaccination adverse events
Asymptomatic & presymptomatic transmission
Waning immunity
Bible
Morality
Logic
Statistics
Experts
Expert consensus
google / existing fact checks
Evaluating information sources
Current US variants
Unvaccinated vs vaccinated COVID cases and deaths
But in the review of about 20,000 COVID-19 cases between Dec. 1 through Jan. 13, when the XBB and XBB.1.5 variants were gaining dominance, researchers found the updated shots helped prevent illness in about half of the people who had previously received two to four doses of the original COVID-19 vaccine, the CDC said.
The article, published in the CDC’s Morbidity and Mortality Weekly Report, showed that among adults aged 18 to 49, the updated vaccine was 48% effective against symptomic infection by XBB/XBB.1.5, compared to 52% against BA.5. For those aged 50 to 64, the effectiveness was 40% compared to 43% against earlier variants.
Among those 65 and older, effectiveness fell to 43% against XBB/XBB.1.5 and 37% against BA.5. Early data show the bivalent shots also reduced the risk of death from COVID-19 by more than twofold in previously vaccinated people and by 13-fold compared with unvaccinated people.
1... Vaccines are predictable.
2... Side effects
3... Long-term safety
4... How mRNA vaccines work (Pfizer & Moderna)
5... How adenovirus vaccines work (Johnson & Johnson)
6... How protein subunit vaccines work (Novavax)
Unlike the natural infection method, vaccines create immunity without causing illness or resulting complications.
Given all of the unknowns--like a region's hospital capacity, or the strength of a person's immune response--choosing the disease over the vaccine is "a very bad decision," she said.
The primary advantage of a vaccine is that it's predictable and safe, she said. "It's been optimally tailored to generate an effective immune response."
...from https://www.nytimes.com/2020/12/05/health/covid-natural-immunity.html
Medical experts say side effects for vaccines are common and are actually an indication the shots are working as intended. Many physicians are advising the public to brace for some stronger-than-usual side effects from the Covid-19 shots, especially after the second dose.
September 12, 2022... The benefits of COVID-19 vaccination continue to outweigh any potential risks.
CDC is providing timely updates on the following adverse events of interest:
· Anaphylaxis after COVID-19 vaccination is rare and has occurred at a rate of approximately 5 cases per one million vaccine doses administered. Anaphylaxis, a severe type of allergic reaction, can occur after any kind of vaccination. If it happens, healthcare providers can effectively and immediately treat the reaction. Learn more about COVID-19 vaccines and allergic reactions, including anaphylaxis.
CDC scientists have conducted detailed reviews of cases of anaphylaxis and made the information available to healthcare providers and the public:
· Thrombosis with thrombocytopenia syndrome (TTS) after J&J/Janssen COVID-19 vaccination is rare and has occurred in approximately 4 cases per one million doses administered. TTS is a rare but serious adverse event that causes blood clots in large blood vessels and low platelets (blood cells that help form clots).
A review of reports indicates a causal relationship between the J&J/Janssen COVID-19 vaccine and TTS. CDC scientists have conducted detailed reviews of TTS
cases and made the information available to healthcare providers and the public:
- Updates on Thrombosis with Thrombocytopenia Syndrome (TTS) [1.3 MB, 39 Pages]
· Guillain-Barré Syndrome (GBS) in people who have received the J&J/Janssen COVID-19 vaccine is rare. GBS is a rare disorder where the body’s immune system damages nerve cells, causing muscle weakness and sometimes paralysis. GBS has largely been reported in men ages 50 years and older.
Based on a recent analysis of data from the Vaccine Safety Datalink, the rate of GBS within the first 21 days following J&J/Janssen COVID-19 vaccination was found to be 21 times higher than after Pfizer-BioNTech or Moderna (mRNA COVID-19 vaccines). After the first 42 days, the rate of GBS was 11 times higher following J&J/Janssen COVID-19 vaccination. The analysis found no increased risk of GBS after Pfizer-BioNTech or Moderna (mRNA COVID-19 vaccines). CDC and FDA will continue to monitor for and evaluate reports of GBS occurring after COVID-19 vaccination and will share more information as it becomes available.
· Myocarditis and pericarditis after COVID-19 vaccination are rare. Myocarditis is inflammation of the heart muscle, and pericarditis is inflammation of the outer lining of the heart. Most patients with myocarditis or pericarditis after COVID-19 vaccination responded well to medicine and rest and felt better quickly. Most cases have been reported after receiving Pfizer-BioNTech or Moderna (mRNA COVID-19 vaccines), particularly in male adolescents and young adults.
A review of vaccine safety data in VAERS from December 2020–August 2021 found a small but increased risk of myocarditis after mRNA COVID-19 vaccines. Over 350 million mRNA vaccines were given during the study period and CDC scientists found that rates of myocarditis were highest following the second dose of an mRNA vaccine among males in the following age groups:
- 12–15 years (70.7 cases per one million doses of Pfizer-BioNTech)
- 16–17 years (105.9 cases per one million doses of Pfizer-BioNTech)
- 18–24 years (52.4 cases and 56.3 cases per million doses of Pfizer-BioNTech and Moderna, respectively)
Multiple studies and reviews of data from vaccine safety monitoring systems continue to show that vaccines are safe. As a result, the agency will refocus enhanced surveillance and safety monitoring efforts toward children and adolescents.
As of September 8, 2022, there have been 1,022 preliminary reports in VAERS among people younger than age 18 years under review for potential cases of myocarditis and pericarditis. Of these, 260 remain under review. Through confirmation of symptoms and diagnostics by provider interview or review of medical records, 672 reports have been verified to meet CDC’s working case definition for myocarditis. See below for counts of verified reports of myocarditis by age group.
5-11 years: 22 verified reports of myocarditis after 21,196,313 doses administered
12-15 years: 348 verified reports of myocarditis after 24,377,482 doses administered
16-17 years: 302 verified reports of myocarditis after 13,362,076 doses administered
As the COVID-19 vaccines are authorized for younger children, CDC and FDA will continue to monitor for and evaluate reports of myocarditis and pericarditis after COVID-19 vaccination and will share more information as it becomes available. Learn more about myocarditis and pericarditis, including clinical considerations, after mRNA COVID-19 vaccination.
· Reports of death after COVID-19 vaccination are rare. FDA requires healthcare providers to report any death after COVID-19 vaccination to VAERS, even if it’s unclear whether the vaccine was the cause. Reports of adverse events to VAERS following vaccination, including deaths, do not necessarily mean that a vaccine caused a health problem. More than 610 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through September 7, 2022. During this time, VAERS received 16,336 preliminary reports of death (0.0027%) among people who received a COVID-19 vaccine. CDC and FDA clinicians review reports of death to VAERS including death certificates, autopsy, and medical records.
Continued monitoring has identified nine deaths causally associated with J&J/Janssen COVID-19 vaccination. CDC and FDA continue to review reports of death following COVID-19 vaccination and update information as it becomes available.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html
Could there be effects decades down the track we haven't predicted? Potentially, but the transient nature of mRNA makes it one of the safer molecules we can use to combat disease.
...from https://www.cnet.com/news/covid-19-vaccines-are-safe-even-if-long-term-data-is-lacking/
There may be very rare side effects that aren't immediately found in clinical trials. But that's due to the extreme rarity of those side effects -- "not because it's a long-term problem," Offit said.
...from https://www.cnn.com/2021/04/28/health/covid-vaccine-myths-debunked/index.html#
Most of the things a vaccine can do to a person's immune system take days, not weeks, months, or years to surface. It is possible for rare complications from a vaccine to surface after 30 days, though they generally take place no more than 42 days afterward, according to federal compensation rules for vaccine injuries. That's because there are three main ways that a body reacts to vaccination, and they all happen relatively fast.
The first is an allergic response to a vaccine's ingredients.
That's "15 to 30 minutes," Creech said, adding: "You have swelling, and we deal with it there in the office."
The second type of vaccine reaction a person can have is an inflammatory response. Most people experience this in the days to week after they're vaccinated.
"That's why a lot of people have arm pain, and fatigue, and fever, and achiness in the day or two after a vaccine," Creech said.
Finally, the third way a vaccine might trigger some issue in the body would be through some kind of abnormal response to vaccination. This can happen as the body is refining its response to a vaccine in the weeks to month after a vaccination. There may be genetic risk factors at play, or medical reasons some people have an unusual immune response at this point, Creech said.
"This is where we might see Bell's palsy after a vaccine, or we might see Guillain-Barré syndrome."
But can those things happen years after a vaccine has been administered?
"There's nothing left to continue to cause problems," Creech said. That's because the vaccine has left the body (for mRNA COVID-19 vaccines, it takes about 36 hours), and the subsequent immune responses it has triggered are all complete.
"If you can get to three months after vaccination, and you haven't had any side effect whatsoever, you're not going to now have a side effect," Creech added.
That's why the Food and Drug Administration requires six months of follow-up safety data on all vaccines before they receive full approval. (For emergency use authorization during a time of crisis, like the pandemic, two months of safety data is, temporarily, allowed.)
· mRNA is made and used in protein production in all cells of our bodies every day. As such, cells have mechanisms in place to ensure that no protein is made in quantities greater than needed. One way this happens is that mRNA has a “poly(A) tail.” In the cytoplasm, this tail ensures mRNA decay. As the mRNA is used to make proteins in the cell, the length of the poly(A) tail decreases, until it is too short for the mRNA to continue being used as a protein blueprint. Once this happens, the mRNA breaks down and is removed as cellular debris. This process limits how long mRNA remains in the cytoplasm — and, therefore, how much protein is produced.
As such, poly(A) tails ensure that the cell breaks down the vaccine mRNA in a timely manner. Likewise, this understanding allows scientists to design vaccine-delivered mRNA in a way that ensures it does not stay in the cell longer than needed to generate immunity.
...from https://www.chop.edu/news/long-term-side-effects-covid-19-vaccine
COVID-19 mRNA vaccines give instructions for our cells to make a harmless piece of what is called the "spike protein." The spike protein is found on the surface of the virus that causes COVID-19.
COVID-19 mRNA vaccines are given in the upper arm muscle. Once the instructions (mRNA) are inside the immune cells, the cells use them to make the protein piece. After the protein piece is made, the cell breaks down the instructions and gets rid of them.
Next, the cell displays the protein piece on its surface. Our immune systems recognize that the protein doesn't belong there and begin building an immune response and making antibodies, like what happens in natural infection against COVID-19.
At the end of the process, our bodies have learned how to protect against future infection. The benefit of mRNA vaccines, like all vaccines, is those vaccinated gain this protection without ever having to risk the serious consequences of getting sick with COVID-19.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html
The Janssen COVID-19 Vaccine is manufactured using a specific type of virus called adenovirus type 26 (Ad26). The vaccine uses Ad26 to deliver a piece of the DNA, or genetic material, that is used to make the distinctive "spike" protein of the SARS-CoV-2 virus. While adenoviruses are a group of viruses that are relatively common, Ad26, which can cause cold symptoms and pink eye, has been modified for the vaccine so that it cannot replicate in the human body to cause illness. After a person receives this vaccine, the body can temporarily make the spike protein, which does not cause disease, but triggers the immune system to learn to react defensively, producing an immune response against SARS-CoV-2.
The Novavax COVID-19 vaccine is a protein subunit COVID-19 vaccine that is authorized for use in the United States under Emergency Use Authorization. Learn more about Novavax COVID-19 vaccine, including who can get it, doses, and ingredients.
How Protein Subunit COVID-19 Vaccines Work
Protein subunit vaccines contain pieces (proteins) of the virus that causes COVID-19. These virus pieces are the spike protein. The vaccine also contains another ingredient called an adjuvant that helps the immune system respond to that spike protein in the future. Once the immune system knows how to respond to the spike protein, the immune system will be able to respond quickly to the actual virus spike protein and protect you against COVID-19.
1. First, protein subunit COVID-19 vaccines are given in the upper arm muscle. After vaccination, nearby cells pick up these proteins.
2. Next, our immune system recognizes that these proteins do not belong there. Another ingredient in the vaccine, the adjuvant, helps our immune system to produce antibodies and activate other immune cells to fight off what it thinks is an infection. This is what your body might do if you got sick with COVID-19.
3. At the end of the process, our bodies have learned how to help protect against future infection with the virus that causes COVID-19. The benefit is that people get this protection from a vaccine, without ever having to risk the potentially serious consequences of getting sick with COVID-19. Many side effects from getting the vaccine are normal signs the body is building protection.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/proteinsubunit.html
June 30, 2022... That means no human trials -- just animal trials and laboratory tests. That might sound scary to some, but regulators already use the same accelerated process to update the flu vaccine each year -- and there is no mechanism by which minor mRNA tweaks will make revised Pfizer and Moderna shots any less safe than the billions of doses administered so far worldwide. Otherwise, the U.S. will miss its fall-winter deadline, and the fast-evolving virus will continue to outrun the vaccines.
As FDA Commissioner Robert Califf recently tweeted, “as we know from prior experience, strain changes can be made without affecting safety.”
...Although these boosters mark the first time Covid-19 shots have been authorized without human testing, according to Poehling, this is the regular approach for the flu vaccine: an updated version is released annually without first undergoing new clinical trials.
...So, Pfizer and Moderna have begun human clinical trials for their updated boosters, with results anticipated later this year. But Poehling says a delay in approval would have been disastrous, as statistical models indicate that it would have caused 9700 deaths and 137,000 hospitalizations.
The new booster will be identical to the original vaccines except it will contain genetic coding for two versions of the protein the virus uses to infect cells — the protein from the original vaccine and proteins from the BA.4 and BA.5 omicron subvariants.
Instead of waiting for results from human trials, the FDA asked the drug companies to initially submit only the results of tests on mice, as NPR reported last week.
In June, an FDA advisory panel composed of independent doctors and scientists voted 19-2 that the agency should approve an Omicron-containing booster shot, and the panelists largely supported making that shot one that contained the BA.4/BA.5 strains, not the earlier Omicron strain for which Pfizer and Moderna had already collected clinical data.
The decision is based on high confidence that the vaccine platforms, which have proven effective against earlier strains, will be effective yet again. It is also based on the hard fact that smaller studies of the vaccines are unlikely to give much information about the known side effects of the vaccines. With the existing vaccines, known issues like myocarditis, an inflammation of the heart that has mostly occurred in young men, are simply too rare to detect in even the largest clinical trials that include tens of thousands of patients. Instead, they have been detected by monitoring of vaccines once they are in broad use.
But rest assured — any booster shot you receive now will be the new one, pharmacists confirmed.
When the U.S. Food and Drug Administration authorized the updated vaccine — called a bivalent vaccine — the agency also changed its authorization for the original vaccine, saying it can no longer be used as a booster for people 12 and older.
The original vaccine will still be used for people getting their initial vaccine doses, a CVS spokesperson confirmed.
With today’s authorization, the monovalent mRNA COVID-19 vaccines are not authorized as booster doses for individuals 12 years of age and older.
...With today’s authorization, the FDA has also revised the EUA of the Moderna COVID-19 Vaccine and the Pfizer-BioNTech COVID-19 Vaccine to remove the use of the monovalent Moderna and Pfizer-BioNTech COVID-19 vaccines for booster administration for individuals 18 years of age and older and 12 years of age and older, respectively. These monovalent vaccines continue to be authorized for use for administration of a primary series for individuals 6 months of age and older as described in the letters of authorization. At this time, the Pfizer-BioNTech COVID-19 Vaccine remains authorized for administration of a single booster dose for individuals 5 through 11 years of age at least five months after completing a primary series of the Pfizer-BioNTech COVID-19 Vaccine.
1... How many adverse events have been reported?
2... Only 1% of adverse events are reported. (Harvard study)
3... How many adverse events are not reported?
4... Healthcare providers are required to report serious adverse events.
5... Serious adverse events are reported more often than minor ones.
6... VAERS cannot determine causality.
Five rare serious adverse events that the CDC is concerned about
Using something purported to be a "Harvard study" (but that is actually a grant report on a project that could not be completed), Elliot performed some truly outrageous back-of-the-envelope math based on that report's claim that VAERS only captures 1% percent of total incidents:
If those numbers are still only 1% of the total adverse reactions ... you can do the math, but that equates to somewhere around 110,000 to 220,000 deaths from the vaccines to date, and a ridiculous number of adverse reactions.
With respect to the 1% figure, extrapolating it to cases of death rests on the false assumption that reporting rates for all adverse events, regardless of severity, are the same. As a spokesperson for the Centers for Disease Control and Prevention (CDC) told Reuters, reporting rates for different types of adverse events vary:
Mild events, like a rash, tend to be reported less frequently than severe events (like a seizure). We have data to show that serious adverse events that occur after vaccination are more likely to be reported than non-serious adverse events. Events such as a sore arm at the injection site might not get reported since they are expected and therefore people don't feel the need to report them.
If your mathematical analysis leads you to claim that there have been 220,000 vaccine caused deaths that have somehow flown under the radar in a climate where six blood clotting incidents paused the distribution of a vaccine, it might make sense to challenge the assumptions that brought you to that "ridiculous number" in the first place.
...from https://www.snopes.com/news/2021/04/16/18-reasons-why/#smg-zone-post-body-4
Are fewer than 1% of vaccine injuries reported to VAERS?
It has long been suspected that reports to VAERS are under-reported, as it is a passive reporting system.
The original claims for under-reporting to VAERS were based on an old study about drug reactions and were not specific to vaccines though.
Is that the Harvard study?
Nope.
"Restructuring at CDC and consequent delays in terms of decision making have made it challenging despite best efforts to move forward with discussions regarding the evaluation of ESP:VAERS performance in a randomized trial and comparison of ESP:VAERS performance to existing VAERS and Vaccine Safety Datalink data. However, Preliminary data were collected and analyzed and this initiative has been presented at a number of national symposia."
Electronic Support for Public Health--Vaccine Adverse Event Reporting System (ESP:VAERS)
They are talking about a report, Electronic Support for Public Health--Vaccine Adverse Event Reporting System (ESP:VAERS), that was conducted at Harvard Pilgrim Health Care, Inc.
"Preliminary data were collected from June 2006 through October 2009 on 715,000 patients, and 1.4 million doses (of 45 different vaccines) were given to 376,452 individuals. Of these doses, 35,570 possible reactions (2.6 percent of vaccinations) were identified."
Electronic Support for Public Health--Vaccine Adverse Event Reporting System (ESP:VAERS)
It is very important to note that all the study found is that all possible reactions, including minor reactions, like pain and fever, are not common.
They didn't actually finish the report to see how commonly those reactions were reported to VAERS.
But we already know that more serious reactions are reported to VAERS much more routinely.
...from https://vaxopedia.org/2019/09/03/percentage-of-reports-to-vaers/#post-40059
Underreporting; FDA does not get most reports of adverse events that occur in the United States. Estimates suggest that FDA receives reports of about 1 to 10 percent of the adverse events that occur.
Also keep in mind that VAERS isn't the only system that helps to monitor vaccine safety. We also have the Vaccine Safety Datalink project, the Clinical Immunization Safety Assessment Network, and the Vaccine Analytic Unit.
...from https://vaxopedia.org/2017/08/26/underreporting-of-side-effects-to-vaers/#caption-attachment-23204
"Underreporting" is one of the main limitations of passive surveillance systems, including VAERS. The term, underreporting refers to the fact that VAERS receives reports for only a small fraction of actual adverse events. The degree of underreporting varies widely. As an example, a great many of the millions of vaccinations administered each year by injection cause soreness, but relatively few of these episodes lead to a VAERS report. Physicians and patients understand that minor side effects of vaccinations often include this kind of discomfort, as well as low fevers. On the other hand, more serious and unexpected medical events are probably more likely to be reported than minor ones, especially when they occur soon after vaccination, even if they may be coincidental and related to other causes.
Like all passive surveillance systems, VAERS is subject to varying degrees of underreporting. The sensitivity of VAERS is affected by the likelihood that parents and/or vaccinees detect an AE; that parents and/or vaccinees bring the event to the attention of their healthcare provider(s); that parents and/or healthcare providers suspect an event is related to prior vaccination; that parents and/or healthcare providers are aware of VAERS; and that parents and/or healthcare providers report the event. The completeness of reporting of AEs associated with certain vaccines varies according to the severity of the event and the specificity of the clinical syndrome to the vaccine.[29,30] Reporting can also be stimulated by media attention on specific AEs.[31]
...from https://www.cdc.gov/vaccines/pubs/surv-manual/chpt21-surv-adverse-events.html#eval-vaers
In their report, Rose and Crawford claim to back up their analysis by citing a CDC study on underreporting levels from previous years (here).
The FDA told Reuters it was aware of the reference but that Rose and Crawford’s paper failed to address "spontaneous adverse event reporting in the context of emergency use authorization (EUA)."
It noted that VAERS reporting levels of adverse events were at their highest after the 2009 H1N1 inactivated pandemic influenza vaccine. The CDC’s study showed 76% of cases of anaphylaxis were captured.
"This suggests that the degree of under reporting in VAERS may be mitigated in the setting of a pandemic where there is a heavy emphasis on vaccine safety," the spokesperson said.
They added that there is also likely to be increased capturing of death reports associated with the COVID-19 vaccine programme, given it has operated on an unprecedented scale under "Emergency Use Authorization" in the United States, which mandates vaccine administrators and manufacturers to report all adverse reactions.
In Kirsch’s paper and committee meeting presentation, Kirsch calculates a so-called "underreporting factor" of adverse reactions by comparing the number of VAERS reports of anaphylaxis (severe allergic reaction) after vaccination with estimates of people vaccinated in the United States. He subsequently applies this number to reported deaths, claiming that more than 150,000 people have died in the United States as a result of COVID-19 vaccines.
Reuters presented these calculations to the FDA, who said: "FDA strongly disagrees with the analysis Mr. Kirsch put forth during the VRBPAC meeting, as we believe the data from VAERS that he referenced were not properly interpreted."
They added: "Although under reporting is a limitation in VAERS with regard to COVID-19 vaccine safety monitoring, there currently is not evidence to suggest it would underestimate the amount of COVID-19 vaccine-related deaths to such a large degree."
As well as VAERS, there are multiple systems the FDA and CDC use to monitor vaccine safety. Given the COVID-19 vaccine is operated under "Emergency Use Authorization" in the United States, vaccine administrators and manufacturers are mandated to report all adverse reactions. This would likely result in increased recording of suspected deaths associated with the COVID-19 vaccine, the FDA spokesperson said.
...from https://www.reuters.com/article/factcheck-coronavirus-usa-idUSL1N2QP18K
A CDC study indicated that, as with all passive surveillance systems, underreporting occurs with VAERS; however, reporting efficiency is higher for severe events than for mild ones (Rosenthal and Chen, 1995). An FDA study found that the reporting rate to VAERS varies substantially by state, but those states that reported the most serious events also reported the most events of lesser severity (Braun, 1997).
The concern of some physicians about potential legal liability for an adverse event following vaccination was cited by some participants as a reason for underreporting in VAERS. Theoretically, this should no longer be the case, because the existence of the National Vaccine Injury Compensation Program (established by federal statute in 1986) has resulted in very few suits filed against physicians for vaccine-related injuries since that time.
...from https://www.ncbi.nlm.nih.gov/books/NBK232983/#_ddd00017_
FDA requires healthcare providers to report any death after COVID-19 vaccination to VAERS, even if it’s unclear whether the vaccine was the cause.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html
The reporting requirements for COVID-19 vaccines are the same for those authorized under emergency use or licensed by the FDA. Healthcare providers who administer COVID-19 vaccines are required to report the following to VAERS:
...· Serious AEs regardless of whether the reporter thinks the vaccine caused the AE. Serious AEs per FDA are defined as:
· Death
· A life-threatening AE
· Inpatient hospitalization or prolongation of existing hospitalization
· A persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions
· A congenital anomaly/birth defect
· An important medical event that based on appropriate medical judgement may jeopardize the individual and may require medical or surgical intervention to prevent one of the outcomes listed above
Underreporting can affect the ability of VAERS to detect very rare events, although this may less [sic] of a concern for clinically serious events as they are more likely to be reported than non-serious events.[29]
...from https://www.cdc.gov/vaccines/pubs/surv-manual/chpt21-surv-adverse-events.html#limitations
Have you heard the claim that only 1% of serious vaccine reactions are reported to VAERS?
That's not true.
That claim is based on an old study about drug reactions and was not specific to vaccines.
We also know that underreporting is less common for more severe adverse reactions than for those that are more mild. For example, one study found that up to 68% of cases of vaccine-associated poliomyelitis (a table injury) were reported to VAERS, while less than 1% of episodes of rash following the MMR vaccine were reported.
...from https://vaxopedia.org/2017/08/26/underreporting-of-side-effects-to-vaers/#caption-attachment-23204
As VAERS does not contain data from unvaccinated populations, VAERS cannot confirm if a vaccine caused something. In other words, without a comparison control group, we don’t know if the adverse events (including deaths) reported to VAERS are actually coincidences that would have happened regardless of the vaccine.
If VAERS contains unverified information and can’t show the causal relationship between an adverse event and a treatment, then what is VAERS’ use? VAERS is only the first step of the surveillance process. As we explained in a previous fact-check, serious adverse events such as death are then investigated by experts from the FDA. In other words, VAERS collects data that are used by authorities as the basis for further investigation.
The key issue is not the URF [underreporting factor]. It is whether it is possible to estimate the number of vaccine-caused deaths from VAERs in the first place (it's not).
And it is what other more rigorous data have to say on the question of vaccine-caused deaths. These can serve as a feasibility check or validation of your VAERs-based estimates. Data like these CMS data covering essentially the entire 65yr+ USA population, lacking the reporting bias problem, and with a natural control group. Data like all-cause death data, including the UK all cause deaths data with deaths split out by vaccination status and age group, as I have posted on recently here and here and here. Data like all-cause death data showing total excess deaths in 2020 and 2021 over time, data that for many countries show the lowest excess death rates in the pandemic during the months when most vaccination was done.
No vaccine manufacturer shall be liable in a civil action for damages arising from a vaccine-related injury or death associated with the administration of a vaccine after October 1, 1988, if the injury or death resulted from side effects that were unavoidable even though the vaccine was properly prepared and was accompanied by proper directions and warnings.
...from https://www.law.cornell.edu/uscode/text/42/300aa-22#tab_default_1
A company can still be sued if they show 'willful misconduct' in the production of their vaccine.
DPT Lawsuits
Through the 1970s and 1980s, the number of lawsuits brought against vaccine manufacturers increased dramatically, and manufacturers made large payouts to individuals and families claiming vaccine injury, particularly from the combined diphtheria-pertussis-tetanus (DPT) immunization. In this environment of increasing litigation, mounting legal fees, and large jury rewards, many pharmaceutical companies left the vaccine business. In fact, by the end of 1984, only one U.S. company still manufactured the DPT vaccine, and other vaccines were losing manufacturers as well.
NCVIA/NCVIP
In October 1986, the U.S. Congress responded to the precarious situation in the vaccine market by passing the National Childhood Vaccine Injury Act (NCVIA). The act included a number of regulations related to informed consent and adverse event reporting. For example, the act required that providers administering certain vaccines provide a Vaccine Information Statement (VIS) to the vaccine recipient or a legal guardian. The VIS lists the risks and benefits of a particular vaccine. The NCVIA also established a system for reporting suspected vaccine-related adverse events. This system, the Vaccine Adverse Event Reporting System (VAERS), is described here. Additionally, the act contained provisions for a program that would fairly and efficiently compensate individuals harmed by certain vaccines that were properly manufactured. Such a system, it was hoped, would stabilize the legal environment for manufacturers, allowing them to limit their liability, better anticipate their legal costs, and reduce potential barriers to research into new vaccines.
Pharmaceutical companies are protected from liability regarding the COVID-19 vaccines. If someone has an allergic reaction or injury from one of the vaccines, they can petition to receive compensation from the Department of Health and Human Services' (HHS) Countermeasures Injury Compensation Program (CICP).
The National Vaccine Injury Compensation Program (VICP), which also falls under the jurisdiction of HHS, has a better record of providing compensation to people who claim injury from a vaccine than CICP but covers vaccines for diseases such as polio and seasonal influenza, not COVID-19.
...There are a few key differences between VICP and CICP.
The Associated Press reported that VICP has paid much more in compensation than CICP has. Only 29 out of 499 people who made claims under CICP received compensation.
Since the late 1980s, VICP has provided $4.4 billion in total compensation, with an average of $570,000 per claim. Since 2005, CICP has provided petitioners, who mostly made claims about the H1N1 swine flu vaccine, $6 million in compensation, with an average of $200,000 per claim. According to theAssociated Press, "payments in most death cases are capped at $370,376" for CICP.
VICP allows individuals to make claims within three years of their first symptom. CICP, on the other hand, allows petitioners only one year from the date of vaccination.
CICP doesn't pay fees for lawyers or expert witnesses or provide awards for suffering or damages; VICP does. VICP also permits appeals all the way to the Supreme Court.
In other words, people who make claims about injuries or allergic reactions to either of the COVID-19 vaccines have less time to make their petitions than people who have filed claims for injuries from vaccines related to the measles or the flu. They also are less likely to receive compensation for injuries from COVID-19 vaccines, and if they do receive compensation, it likely will be a smaller amount.
"There is an irresolvable tension between speed and safety," said Dr. Gregory Poland, the head of Mayo Clinic's Vaccine Research Group. "Efficacy is pretty easy to figure out. It's safety that's the issue."
...from https://khn.org/news/these-secret-safety-panels-will-pick-the-covid-vaccine-winners/#
Trials were designed such that clinical phases are overlapping and trial starts are staggered, with initial phase I/II trials followed by rapid progression to phase III trials after interim analysis of the phase I/II data.
...from https://www.nature.com/articles/s41586-020-2798-3#figure-2-desc
Moving at "warp speed" allows "a very rapid development without inappropriate corners being cut," Slaoui said. "All the risk taken is financial, logistical, and resourcing, but not on safety or efficacy." Bureaucratic obstacles have been loosened, removing the usual gaps between different phases of clinical trials and saving precious time, he said.
The vaccine science would not have produced such fast results without this funding, she says. "It didn't happen with Ebola, which was devastating communities in Africa [in 2014--16]" -- and Ebola vaccines accordingly took longer to develop. The money only materialized this time because all countries, including wealthy ones, faced economic devastation: suggesting that the development of future vaccines, including for existing diseases such as malaria, will not be as speedy. "Unless you put in the money, there's no way to accelerate," says Rappuoli.
...from https://www.nature.com/articles/d41586-020-03626-1#Fig2
Research history:
The basic research on DNA vaccines began at least 25 years ago, and RNA vaccines have benefited from 10--15 years of strong research, she says, some aimed at developing cancer vaccines. The approach has matured just at the right time; five years ago, the RNA technology would not have been ready.
...from https://www.nature.com/articles/d41586-020-03626-1#Fig2
During the SARS1 (SARS-CoV-1) outbreak 18 years ago, researchers started looking at that virus, and other coronaviruses, and found a really promising vaccine target on the virus cell surface -- which is a protein called spike. That protein is what binds to human cells and leads to an infection.
So about 10 years ago the science wheels started churning out strategies to vaccinate against SARS1. Unfortunately, funding dried up for SARS1 as that virus never made its way to the U.S., so a vaccine didn't actually get developed. However, the research on the virus and ideas of how to vaccinate against it were already available.
Thankfully SARS2 (SARS-CoV-2, our current situation) uses almost the exact same version of that protein to infect cells and uses the exact same receptor on human cells. Due to these similarities, scientists were able to pick up where they left off, which sped up the process dramatically.
Further, vaccination strategies have improved significantly in the last 10-plus years, particularly in the past couple of years with the mRNA technology that Moderna and Pfizer have utilized. All of these companies basically just took the DNA or RNA backbone of a vaccine that they had already built and plugged in the SARS2 spike protein's genetic information.
...from https://www.sltrib.com/opinion/commentary/2020/11/20/allison-weis-covid/#navbar
Researchers have been developing and researching an mRNA vaccine platform for over 10 years. After SARS-CoV-2 was sequenced, it took just a few days to make the mRNA vaccine candidates. The spike protein's genetic code was plugged into preexisting technology with an already working process that had been evaluated for other vaccine uses, such as in the fight against dengue.
...from https://www.nebraskamed.com/COVID/were-the-covid-19-vaccines-rushed#block-mainpagecontent
The third vaccine to show efficacy in phase III clinical trials in November, made by the pharmaceutical firm AstraZeneca with the University of Oxford, UK, does not use mRNA. Instead, a viral vector (or carrier) holds extra genetic material that codes for the SARS-CoV-2 spike protein. This, too, benefited from years of research to select the vector; in this case, the firm chose a modified form of adenovirus isolated from chimpanzee stool. Advances in conventional vaccines such as these have also come from research on SARS, MERS, Ebola and malaria, says Beate Kampmann, director of the Vaccine Centre at the London School of Hygiene & Tropical Medicine, and such approaches remain cheaper than using mRNA.
...from https://www.nature.com/articles/d41586-020-03626-1#Fig2
For the Pfizer-BioNTech COVID-19 Vaccine, the FDA amended the EUA to include use of the vaccine in individuals 6 months through 4 years of age. The vaccine had been authorized for use in individuals 5 years of age and older.
A pivotal Phase 2/3 trial of more than 43,000 healthy participants around the world (NCT04368728) published in NEJM,
...from https://www.raps.org/news-and-articles/news-articles/2020/3/covid-19-vaccine-tracker
a Phase 2 trial of 960 participants in China in conjunction with Shanghai Fosun Pharmaceutical (NCT04649021),
a Phase 1/2 trial in the US and Germany of 200 healthy participants between aged 18-55 years (NCT04380701),
and a combined Phase 1/2 trial of 160 participants (NCT04588480) in Japan.
For the Moderna COVID-19 Vaccine, the FDA amended the emergency use authorization (EUA) to include use of the vaccine in individuals 6 months through 17 years of age. The vaccine had been authorized for use in adults 18 years of age and older.
In the pivotal Phase 3 trial of 30,000 participants at high risk for COVID-19, participants received a 100 µg dose of mRNA-1273 and another 4 weeks later or placebo injections and then be followed for up to 2 years (COVE trial; NCT04470427). Moderna posted the full trial protocol for COVE on 17 September.
Previously, a Phase 1 trial (NCT04283461) of 105 healthy participants provided the basis for Moderna's investigational new drug application (IND), which was successfully reviewed by the FDA and set the stage for Phase 2 testing.
A Phase 2 trial of 600 healthy participants evaluating 25 µg, 100 µg, and 250 µg dose levels of the vaccine was completed.
(NCT04405076). Moderna has also launched a Phase 2/3 trial testing mRNA-1273 in about 3,000 adolescents 12 years to less than 18 years old (NCT04649151).
...from https://www.raps.org/news-and-articles/news-articles/2020/3/covid-19-vaccine-tracker
The data also show that the vaccine's known and potential benefits outweigh its known and potential risks, supporting the company's request for the vaccine's use in people 18 years of age and older.
The available safety data to support the EUA include an analysis of 43,783 participants enrolled in an ongoing randomized, placebo-controlled study being conducted in South Africa, certain countries in South America, Mexico, and the U.S. The participants, 21,895 of whom received the vaccine and 21,888 of whom received saline placebo, were followed for a median of eight weeks after vaccination. The most commonly reported side effects were pain at the injection site, headache, fatigue, muscle aches and nausea. Most of these side effects were mild to moderate in severity and lasted 1-2 days.
As part of the authorization, the FDA notes that it is mandatory for Janssen Biotech Inc. and vaccination providers to report the following to the Vaccine Adverse Event Reporting System (VAERS) for Janssen COVID-19 Vaccine: serious adverse events, cases of Multisystem Inflammatory Syndrome and cases of COVID-19 that result in hospitalization or death.
Today, the U.S. Food and Drug Administration issued an emergency use authorization (EUA) for the Novavax COVID-19 Vaccine, Adjuvanted for the prevention of COVID-19 caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in individuals 18 years of age and older.
...The safety of the vaccine was assessed in approximately 26,000 clinical trial participants who received the vaccine and approximately 25,000 who received placebo. The most commonly reported side effects by vaccine recipients included pain/tenderness, redness and swelling at the injection site, fatigue, muscle pain, headache, joint pain, nausea/vomiting and fever. Approximately 21,000 vaccine recipients had at least two months of safety follow-up after their second dose.
The Moderna COVID-19 Vaccine, Bivalent is authorized for use as:
· a single booster dose in children 6 months through 5 years of age at least two months after completion of a primary series with the monovalent Moderna COVID-19 Vaccine.
· a single booster dose in individuals 6 years of age and older at least two months after completion of either primary vaccination with any authorized or approved COVID-19 vaccine, or receipt of the most recent booster dose with any authorized or approved monovalent COVID-19 vaccine.
The Pfizer-BioNTech COVID-19 Vaccine, Bivalent, when administered as a booster dose, is authorized for use as:
· a single booster dose in children 6 months through 4 years of age at least 2 months after completion of primary vaccination with three doses of the monovalent Pfizer-BioNTech COVID-19 Vaccine.
· a single booster dose in individuals 5 years of age and older at least two months after completion of either primary vaccination with any authorized or approved COVID-19 vaccine or receipt of the most recent booster dose with any authorized or approved monovalent COVID-19 vaccine.
The safety data accrued with the bivalent vaccine (original and omicron BA.1) and with the monovalent Moderna COVID-19 Vaccine are relevant to the Moderna COVID-19 Vaccine, Bivalent because these vaccines are manufactured using the same process.
The clinical study that evaluated the safety of a booster dose of the bivalent vaccine (original and omicron BA.1) included approximately 800 participants 18 years of age and older who had previously received a two dose primary series and one booster dose of the monovalent Moderna COVID-19 Vaccine, and then at least 3 months later, received a second booster dose with either the monovalent Moderna COVID-19 Vaccine or Moderna’s investigational bivalent COVID-19 vaccine (original and omicron BA.1).
...The safety data accrued with the bivalent vaccine (original and omicron BA.1) and with the monovalent Pfizer-BioNTech COVID-19 Vaccine are relevant to Pfizer-BioNTech COVID 19 Vaccine, Bivalent because these vaccines are manufactured using the same process.
The clinical study that evaluated the safety of a booster dose of the bivalent vaccine (original and omicron BA.1) included approximately 600 participants greater than 55 years of age who had previously received a 2-dose primary series, one booster dose of the monovalent Pfizer-BioNTech COVID-19 Vaccine, and then 4.7 to 13.1 months later, received a second booster dose of either the monovalent Pfizer-BioNTech COVID-19 Vaccine or Pfizer-BioNTech’s investigational bivalent COVID-19 vaccine (original and omicron BA.1).
Vaccines reduce infections.
Immunity wanes following both infection and vaccination.
"Vaccines decrease your risk of COVID-19. They don't make you immortal."
People with vaccine breakthrough infections may spread COVID-19 to others.
With more people getting vaccinated, and protection declining over time since the initial vaccination series, breakthrough cases are to be expected, experts concurred.
Of course there are people who catch COVID-19 after being fully vaccinated. No vaccine is 100% effective; so we always knew that this would happen. Again, this is the Nirvana fallacy, in which antivaxxers suggest that if a vaccine isn't 100% effective it's crap.
Among 1,228,664 persons who completed primary vaccination during December 2020--October 2021, severe COVID-19--associated outcomes (0.015%) or death (0.0033%) were rare. Risk factors for severe outcomes included age ≥65 years, immunosuppressed, and six other underlying conditions. All persons with severe outcomes had at least one risk factor; 78% of persons who died had at least four.
...from https://www.cdc.gov/mmwr/volumes/71/wr/mm7101a4.htm?s_cid=mm7101a4_w
Vaccine effectiveness against Omicron
Low levels of vaccination can also contribute to new variants that could be more lethal or have more immune-escape capabilities, Pekosz says.
...from https://publichealth.jhu.edu/2022/omicron-qa-making-some-sense-of-the-messiness-of-this-moment
Unvaccinated vs vaccinated COVID cases and deaths
...In April, after months of public-health experts cautiously promoting the merits of vaccination, CDC Director Rochelle Walensky cited new real-world data of the shots' effectiveness to jubilantly proclaim that "vaccinated people do not carry the virus.
...An outbreak in Provincetown, Massachusetts--in which 74 percent of the 469 cases were in the fully vaccinated--forced the CDC to update its mask guidance and issue a sad and sobering warning: Vaccinated people infected with the SARS-CoV-2 Delta variant can be just as contagious as unvaccinated people.
...To spread the coronavirus, you have to have the coronavirus. And vaccinated people are far less likely to have the coronavirus--period.
"From a clinical perspective, we expect to see the number of breakthrough cases go up as more people get vaccinated. It is like what we saw with seat belt use years ago. As the number of people wearing seatbelts increased, the number of car accidents involving people wearing seatbelts went up. However, the overall fatality rate from car accidents dropped. Your chances of dying in a car accident drop dramatically if you wear a seatbelt. So too, your chances of dying from COVID-19 drop substantially if you are fully vaccinated," Acting PA Physician General Denise Johnson said.
Clearly, the vaccines are impressively effective. Still, overall, more vaccinated Israelis were in the hospital than unvaccinated ones. This is a natural consequence of the fact that if you prioritize the most vulnerable people for vaccination -- which is what you should do -- then vaccinated people will be disproportionately drawn from the vulnerable population. That means more of them than you might otherwise expect will end up sick. (Since Aug. 15, the picture has changed somewhat: Israel now has more unvaccinated hospitalized patients than vaccinated hospitalized patients, possibly related to the rollout of booster doses at the end of July.)
Positive cases have been climbing in Vermont in recent weeks despite the state's having one of the highest vaccination rates against the virus in the U.S. Cases rose last year around this time as well as people spent more time indoors, but the state still enjoyed one of the lowest case rates in the country then.
...Unvaccinated Vermonters are still the people getting sick and being hospitalized at the highest rates.
...The highly contagious delta variant is still one of the main factors affecting cases in Vermont, as it has been for most of the year, Levine said. The variant has even been able to spread among vaccinated people.
...There were fewer Vermonters who got sick early in the pandemic, but this also meant that fewer residents were able to build up any level of immunity from having the virus.
...Vermont's success in vaccinating its residents quickly, starting with the oldest Vermonters, means immunity among the highest-risk people in the state is likely waning now, Levine said.
...Finally, Vermonters are also traveling more and hosting visitors, often taking part in indoor activities, more frequently than they would have at this time last year. They are also wearing masks less often.
...from https://news.yahoo.com/highly-vaccinated-vermont-more-covid-152537112.html
The new guidance is likely to open the door to confusion, since there is no surefire way for businesses or others to distinguish between those who are fully vaccinated and those who are not.
...And while some people still get COVID-19 despite being vaccinated, Walensky said that's rare and cited evidence that those infections tend to be milder, shorter and harder to spread to others. If people who are vaccinated do develop COVID-19 symptoms, they should immediately put their mask back on and get tested, she said.
...from https://apnews.com/article/coronavirus-masks-cdc-guidelines-9d10c8b5f80a4ac720fa1df2a4fb93e5#
There simply aren't enough people who have been vaccinated yet.
...from https://uihc.org/health-topics/3-reasons-why-we-need-wear-mask-after-covid-19-vaccination#row-13556
In indoor public spaces, the vaccination status of other people or whether they are at increased risk for severe COVID-19 is likely unknown. Therefore, fully vaccinated people should continue to wear a mask that fits snugly against the sides of your face and doesn't have gaps, cover coughs and sneezes, wash hands often, and follow any applicable workplace or school guidance.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html#
Paul to Fauci: Given that no scientific studies have shown significant numbers of reinfections of patients previously infected, or previously vaccinated, what specific studies do you cite to argue that the public should be wearing masks well into 2022?
Fauci to Paul: In the South African study, conducted by J&J, they found that people who were infected with wild type and were exposed to the variant in South Africa--the 3.5.1--it was if they had never been infected before--they had no protection.
...from https://www.youtube.com/watch?v=RrpEOg1cFj0&list=PLEb9Wh_GlgF5VUpBmG1G_4WkgoGRdWT6u
Before approving the Moderna and Pfizer vaccines, the FDA asked the vaccine manufacturers only whether their products protect people from COVID-19 symptoms. They didn't ask if the vaccines stop people who've been vaccinated from nevertheless spreading the virus to others. The emergency authorizations by the FDA that have allowed distribution of the two new vaccines cite only their ability to keep you -- the person vaccinated -- from becoming severely sick with COVID-19.
With cases and deaths surging throughout the U.S., the people who are treating COVID-19 patients really want you to continue to wear a mask, keep your distance and wash your hands, even if you've been vaccinated, until the research on shedding has yielded some answers. Dr. Carlos del Rio of Emory University says he knows taking precautions can be taxing, but he urges us all to hang on and keep it up.
"It's not like you'll need to wear a mask for the rest of your life," he says. "You need to wear your mask until we have the data, and we're trying to get the answers as fast as we can."
Until proven otherwise, people should consider asymptomatic infections and transmission to be a possibility. "There's a concern that people could get the vaccine and feel like they are safe, but they could be actually infected with the virus and carry it in their nasal passages and in their airways. And because they're feeling safe, they might be less cautious and actually spread the disease," said Boslett. With this in mind, health officials are urging everyone, even people who have received the vaccination, to continue to wear masks, stay six feet apart from people not in their own household and to wash their hands frequently.
Usually, getting infected with any given virus produces broader immunity than getting vaccinated against it. That’s because when you’re infected, your immune system is exposed to the entire virus and can generate defenses against any parts of it. That response is typically more layered than the limited one provoked by vaccines.
However, studies of people vaccinated against COVID-19 do not bear that out. “When we compare vaccinated people vs. those who had one less vaccine and then a breakthrough infection, people with the breakthrough infection should be better protected against another infection, but they are not,” says Sahin. “The data show that adding one vaccine dose provides better protection than adding an infection.”
...from https://time.com/6240499/how-covid-19-immunity-works-vaccines-infections/
A systematic review and meta-analysis including data from three vaccine efficacy trials and four observational studies from the US, Israel, and the United Kingdom, found no significant difference in the overall level of protection provided by infection as compared with protection provided by vaccination; this included studies from both prior to and during the period in which Delta was the predominant variant [79]. In this review, the randomized controlled trials appeared to show higher protection from mRNA vaccines whereas the observational studies appeared to show protection to be higher following infection.
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/vaccine-induced-immunity.html
Recovery from many viral infectious diseases is followed by a period of infection-induced immunologic protection against reinfection. This phenomenon is widely observed with many respiratory viral infections, including both influenza and the endemic coronaviruses, for which acquired immunity also wanes over time making individuals susceptible to reinfection.
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/vaccine-induced-immunity.html
Protection against COVID-19 after 2 doses of mRNA vaccine wanes, but little is known about durability of protection after 3 doses.
COVID is high-risk.
COVID vaccines are low-risk.
Masks are no-risk for adults.
The findings highlight an advantage bestowed by natural infection rather than vaccination, but the authors caution that the benefits of stronger memory B cells do not outweigh the risk of disability and death from COVID-19.
It is true that natural infection almost always causes better immunity than vaccines. Whereas immunity from disease often follows a single natural infection, immunity from vaccines usually occurs only after several doses. However, the difference between vaccination and natural infection is the price paid for immunity:
To Mr. Paul's point: Natural immunity from the coronavirus is fortunately quite strong. A vast majority of people infected produce at least some antibodies and immune cells that can fight off the infection. And the evidence so far suggests that this protection will persist for years, preventing serious illness, if not reinfection.
But there is a "massive dynamic range" in that immune response, with a 200-fold difference in antibody levels.
In people who are only mildly ill, the immune protection that can prevent a second infection may wane within a few months. "Those people might benefit more from the vaccine than others would," said Bill Hanage, an epidemiologist at the Harvard T.H. Chan School of Public Health.
With a vaccine, everyone gets the same dose. "We know the dose that is being administered, and we know that that dose is effective at eliciting an immune response," Dr. Gommerman said. "So that becomes a variable that's taken off the table when you get the vaccine."
...from https://www.nytimes.com/2020/12/05/health/covid-natural-immunity.html#
What is already known about this topic?
Data are limited regarding the risks for SARS-CoV-2 infection and hospitalization after COVID-19 vaccination and previous infection.
What is added by this report?
During May--November 2021, case and hospitalization rates were highest among persons who were unvaccinated without a previous diagnosis. Before Delta became the predominant variant in June, case rates were higher among persons who survived a previous infection than persons who were vaccinated alone. By early October, persons who survived a previous infection had lower case rates than persons who were vaccinated alone.
What are the implications for public health practice?
Although the epidemiology of COVID-19 might change as new variants emerge, vaccination remains the safest strategy for averting future SARS-CoV-2 infections, hospitalizations, long-term sequelae, and death. Primary vaccination, additional doses, and booster doses are recommended for all eligible persons. Additional future recommendations for vaccine doses might be warranted as the virus and immunity levels change.
Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
...We conducted a retrospective observational study comparing three groups: (1)SARS-CoV-2-naďve individuals who received a two-dose regimen of the BioNTech/Pfizer mRNA BNT162b2 vaccine, (2)previously infected individuals who have not been vaccinated, and (3)previously infected and single dose vaccinated individuals.
...from https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full
The study period predated the identification of Omicron, which might upend the authors' conclusions, says Amit Huppert, a mathematical biologist at the Gertner Institute for Epidemiology and Health Policy Research in Tel HaShomer, Israel, and a co-author of the study. "Two weeks ago, I might have said 'don't deal with the recovered population in their first year of recovery and focus your efforts on vaccinating other populations'," he says. But the latest data showing that reinfections and breakthrough infections are more likely with the Omicron variant suggest that hybrid or boosted immunity will be key to preventing severe infection, he adds.
Dowdy says although these data will help public health officials to identify the most effective vaccine regimen, they should not have any bearing on policy today.
Huppert agrees. "At the end of the day, these are subtleties," he says. "The main message is get vaccinated."
But "suspected but unconfirmed" doesn't refer to participants who were probably sick with COVID-19. On the contrary, it refers to participants who reported various symptoms, such as a cough or a sore throat, and then took a PCR test--and then that test came back negative.
With 20 times more suspected than confirmed cases, this category of disease cannot be ignored simply because there was no positive PCR test result.
We are very concerned about data mentioned exclusively in an FDA briefing document (p.42) describing 3410 'suspected but unconfirmed' cases of COVID-19, including 1594 vaccine and 1816 placebo subjects. This statistic points to a critical, but missing, datapoint: the number tested for COVID-19 in each group. As per the study protocol (p89) all subjects should have been tested. However, neither the published manuscript nor the FDA document describes how many in each group were tested.
...from https://www.thennt.com/review-covid-analysis-2020/#staticpage
As described in Section 8.13, page 88/137 of the protocol, they did this by instructing subjects to immediately contact the site for a SARS-CoV-2 PCR test if they experienced any of the following symptoms anew that COULD indicate potential COVID-19: fever, cough, shortness of breath, chills, muscle pain, sore throat, loss of taste/smell, diarrhea, and vomiting. The protocol states that anyone reporting one of these symptoms (except within 7 days of receiving shot) is a suspected COVID-19 patient who should immediately arrange a potential COVID-19 illness visit to receive a PCR test to determine if they are infected with the SARS-CoV-2 virus or not. Those who receive a positive PCR test are "confirmed COVID-19 cases" that are included in the primary efficacy analysis, and those whose PCR test is negative (or if done multiple times, repeatedly negative) are "suspected but unconfirmed COVID-19 cases."
Thus, it is clear that "suspected but unconfirmed COVID-19 cases" are all of those who reported one of those flu-like symptoms but whose SARS-CoV-2 PCR test came back negative. [Emphasis in the original]
The only reason why it might be appropriate to include these in the efficacy endpoint are if one believes that most or all of them are false negative test results, which Doshi implies is a possibility given his statement "If many or most of these suspected cases were in people who had a false negative PCR test result, this would dramatically decrease vaccine efficacy." However, it is completely implausible that many or most of these 3410 were COVID-19 cases with false negative SARS-CoV-2 PCR tests, given that for this to be the case it would have to be true that:
· 3410/~30,000 = ~11.4% of study participants were infected with symptomatic COVID-19 within ~2 months during a time in which the confirmed case rate was ~0.5%/month in USA.
· Since "suspected case" implies symptoms were reported, this would not even include asymptomatic cases, which are estimated to be 50-80% of all cases, suggesting that the true infection rate in the population of trial subjects would then be ~20-50%, which is clearly implausible.
· the false negative rate would have to be FAR beyond any documented or reasonably posited levels. The nominal false negative rate for the PCR test mentioned in the Pfizer protocol is 2% (see table 3 of FDA report for this PCR test), which would suggest that 3/3410 of these suspected cases were in fact false negative COVID-19 cases, and the updated efficacy would be (174-10)/174 x 100 =93.9% if we pessimistically assumed the vaccine efficacy was 0% for all false negative cases. Even if we assumed the FNR was 10x higher than reported, say 20%, this would mean we expected 43/3410 of these suspected cases to in fact be false negative COVID-19 cases, which would correspond to an updated efficacy of (183-29)/183 x 100 =84.2% if were pessimistically assumed the vaccine efficacy was 0% for all false negative cases. Even assuming a high 20% FNR, this would only result in ~1% of the 3410 being false negatives, obviously far short of "many or most".
· The high false negative rates that would have to be assumed to propose "many or most of the 3410" are false negatives would imply that essentially everyone in the USA has already been infected with SARS-CoV-2 given the >24 million confirmed cases in the USA for which the individual received a PCR test and a positive test result was obtained.
· To expect "many or most" of these to be false positive COVID-19 cases also implies that there were very few cases of common cold, seasonal allergies, or food-based nausea or diarrhea in this cohort of ~30,000 patients for the study duration that may have produced any of those common flu-like symptoms outside of COVID-19.
It is obvious that to suggest that "many or most" of these are false negative COVID-19 cases is patently absurd.
Like other COVID-19 vaccines, Novavax does not cause COVID-19 infection. It can't get you sick. This vaccine doesn't contain either live or inactivated virus.
...from https://www.nebraskamed.com/COVID/moths-and-tree-bark-how-the-novavax-vaccine-works
Some vaccines, such as the measles or oral polio vaccines, contain a weakened form of the live virus, and in very rare cases these can cause disease. "But this isn't one of those," said Boslett. "The mRNA vaccines just contain a message that encodes the spike protein. It is not a live virus, so there's no chance that the vaccine can give you COVID."
The J&J shot is based on a different technology than the Moderna and Pfizer vaccines. Those use mRNA, or messenger RNA, to deliver bits of genetic code to cells. This code serves as a sort of instruction sheet -- telling cells how to make a harmless piece of the spike protein that sticks out of the surface of the coronavirus. The immune system then learns to recognize the spike protein and fight it.
The Johnson & Johnson vaccine, by contrast, is what's known as a viral vector vaccine -- the same technology that's been proven safe and effective in creating an Ebola vaccine and others currently in the works. Basically, Johnson & Johnson started with an adenovirus, which causes the common cold, and modified it so it can't make anybody sick. They then used this harmless cold virus to deliver the genetic blueprint of the protein spike to cells, so the immune system will learn to recognize that spike when it runs into the coronavirus.
To be clear, the J&J vaccine "can't give you the cold virus, and it definitely cannot give you COVID," says Dr. Cassandra Pierre, an infectious disease specialist and acting hospital epidemiologist at Boston Medical Center.
How mRNA vaccines work (Pfizer & Moderna)
How adenovirus vaccines work (Johnson & Johnson)
How protein subunit vaccines work (Novavax)
There are four approved or authorized vaccines in the United States used to prevent COVID-19. Pfizer-BioNTech and Moderna are COVID-19 mRNA vaccines. You can also get the Novavax COVID-19 protein subunit vaccine. Otherwise, you may get Johnson & Johnson’s Janssen (J&J/Janssen) COVID-19 viral vector vaccine in some situations.
These vaccines are given as a shot in the muscle of the upper arm or in the thigh. None of them affect or interact with our DNA in any way.
The genetic material delivered by mRNA vaccines never enters the nucleus of your cells, which is where your DNA is kept. Viral vector COVID-19 vaccines deliver genetic material to the cell nucleus to allow our cells to build protection against COVID-19. However, the vector virus does not have the machinery needed to integrate its genetic material into our DNA, so it cannot alter our DNA.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/facts.html#languageDropDownMenu
The use of fetal tissue in vaccine development is the practice of researching, developing, and producing vaccines through growing viruses in cultured (laboratory-grown) cells that were originally derived from human fetal tissue.[1] Since the cell strains in use originate from abortions,[2] there has been opposition to the practice and the resulting vaccines on religious and moral grounds.[1][3][4]
The vaccines do not contain any of the original fetal tissue or cells or cells derived from fetal materials.[5] Although the vaccine materials are purified from cell debris, traces of human DNA fragments remain.[6][7][8] The cell lines continue to replicate on their own and no further sources of fetal cells are needed.[5]
The Catholic Church has encouraged its members to use alternative vaccines, produced without human cell lines, if possible. However, the Vatican has clarified that "all vaccinations recognized as clinically safe and effective can be used in good conscience, with the certain knowledge that the use of such vaccines does not constitute formal cooperation with the abortion".
...from https://en.wikipedia.org/wiki/Use_of_fetal_tissue_in_vaccine_development#mw-content-text
The Archdiocese of New Orleans, in light of guidance from the Vatican, the United States Conference of Catholic Bishops, and The National Catholic Bioethics Center affirm that though there was some lab testing that utilized the abortion-derived cell line, the two vaccines currently available from Pfizer and Moderna do not rely on cell lines from abortions in the manufacturing process and therefore can be morally acceptable for Catholics as the connection to abortion is extremely remote.
It is under the same guidance that the archdiocese must instruct Catholics that the latest vaccine from Janssen/Johnson & Johnson is morally compromised as it uses the abortion-derived cell line in development and production of the vaccine as well as the testing.
We maintain that the decision to receive the COVID-19 vaccine remains one of individual conscience in consultation with one's healthcare provider. We also maintain that in no way does the Church's position diminish the wrongdoing of those who decided to use cell lines from abortions to make vaccines. In doing so, we advise that if the Moderna or Pfizer vaccine is available, Catholics should choose to receive either of those vaccines rather than to receive the new Johnson & Johnson vaccine because of its extensive use of abortion-derived cell lines.
Vaccine effectiveness is an estimate of the risk of getting infected.
Vaccination reduces all the risks of COVID-19, including death.
The survival rate of COVID-19 is an estimate of the risk of death if you get infected.
Infection exposes you to all the risks of COVID-19, including death.
Vaccines are statistically safer than getting infected.
The best way to prevent illness is to avoid being exposed to this virus.
...from https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html
There has been no evidence that the COVID-19 vaccines weaken the immune system.
"After COVID-19 vaccination, your immune system is just as able to fight off infections by cold or flu viruses, and it will be better prepared to protect you against COVID-19."
The vaccines that children receive in the first two years of life are just a drop in the ocean when compared with the tens of thousands of environmental challenges that babies successfully manage every day.
...By the end of the first week of life, the child's skin, nose, throat and intestines are covered with tens of thousands of different bacteria.
40% of patients with weakened immune system mount lower response to vaccines
...In early January, the CDC issued guidelines stating that those who are moderately or severely immunocompromised and have difficulty retaining immunity should get a booster and additional primary shot, for a total of 4 shots.
...from https://www.healthline.com/health-news/why-a-4th-covid-19-shot-likely-wont-provide-more-protection
"Despite what some people have incorrectly reported, Dr. Cavaleri has never said or implied that the repeated administration of boosters would weaken the immune system in any way," Zala Grudnik, a spokesperson for the agency, said in an email. "What he said is that repeated administration of boosters might lead to the immune response to the vaccine being lower, which means the vaccines could become less effective."
I HAVE AN AUTOIMMUNE DISEASE -- AM I AT RISK OF EXPERIENCING A FLARE-UP FROM THE VACCINE?
There is a risk that flare-ups may occur. That being said, it has been observed that people living with autoimmune and inflammatory conditions are at higher risk of experiencing severe symptoms from a COVID-19 infection. Due to this concern, the American College of Rheumatology has stated that "the benefit of COVID-19 vaccination outweighs any small, possible risks for new autoimmune reactions or disease flare after vaccination."
...from https://www.autoimmuneinstitute.org/vaccine-autoimmune-disease-faq/
Explaining why the common cold may be in wider circulation this year, he added: "Last winter we were in lockdown and social mixing, especially indoors, was very limited. This was very effective in limiting the spread of the coronavirus but also had other consequences. At the same time, it reduced our exposure to common cold viruses. Cases were very low indeed, meaning that the annual immunity top-up we normally received through virus infection did not occur.
"Unfortunately, our natural protection to the common cold will have declined to some degree, and this is reflected in the reports of increased severity of symptoms. But this is not at all due to impacts of the COVID-19 vaccination on our immune systems."
A spokesperson for the University of Oxford COVID-19 Vaccine Team said: "There is no truth at all that vaccines weaken the immune system and that this causes death. This suggestion goes against every scientific principle of vaccination."
Scientists are watching in real time as original antigenic sin plays out against the coronavirus — and debating how it will influence future vaccine strategy. Contrary to its biblical thunderclap of a name, the phenomenon is nuanced — more often beneficial or neutral than harmful.
...But not all “sin” is created equal. For a virus like dengue, original antigenic sin can be harmful. For flu, it may help in some scenarios and hinder immunity in others. The limited data has left experts in a familiar place during this pandemic: watching what happens next.
...from https://www.washingtonpost.com/health/2022/08/22/coronavirus-immune-response-boosters/
Although antibody studies reveal the telltale signature of imprinting, Gostic says, there is little evidence that those signatures affect people’s susceptibility to illness. Even if it lessens protection, says Boyton, “there’s no evidence that it causes harm, makes a worse immune response, or makes you more sick” compared with people who are unvaccinated or haven’t been infected.
How many cases of myocarditis have been reported following vaccination?
In particular, the CDC emphasized that young men, between the ages of 12--39 years, who may be at increased risk for myocarditis, should consider this extended time series.
"Extending the interval between the first and second mRNA vaccine dose to 8 weeks might reduce the risk [of myocarditis]," the agency wrote.
The original waiting period between the first and second dose is still recommended for immunocompromised Americans, adults over the age of 65, and those who may need more rapid protection, due to an increased risk of infection or severe disease.
An 8-week interval between the first and second primary series doses of Moderna, Novavax, and Pfizer-BioNTech COVID-19 vaccines may be optimal for some people as it may reduce the small risk of myocarditis and pericarditis associated with these COVID-19 vaccines.
COVID-19 vaccines are FDA-approved or FDA-authorized for a 3-week (Novavax and Pfizer-BioNTech) or 4-week (Moderna) interval between the first and second dose. A 3- or 4-week interval continues to be the recommended interval for people who are moderately or severely immunocompromised, adults ages 65 years and older, and in situations when the fullest possible protection needs to be achieved sooner (e.g., increased concern about COVID-19 community levels or an individual’s higher risk for severe disease).
Moderna, Novavax, and Pfizer-BioNTech COVID-19 vaccines are safe and effective at the FDA-approved or FDA-authorized intervals, but a longer interval may be considered for some populations. While absolute risk remains small, an elevated risk for myocarditis and pericarditis has been observed among mRNA COVID-19 vaccine recipients, particularly in males ages 12–39 years (see COVID-19 vaccination and myocarditis and pericarditis). Cases of myocarditis and pericarditis were identified in clinical trials of Novavax COVID-19 Vaccine and through passive surveillance during post-authorization use outside the United States.
The risk of vaccine-associated myocarditis and pericarditis might be reduced by extending the interval between the first and second primary series doses of these vaccines. Some studies in adolescents (ages 12–17 years) and adults have shown the small risk of myocarditis and pericarditis associated with mRNA COVID-19 vaccines might be reduced and peak antibody responses and vaccine effectiveness may be increased with an interval longer than 4 weeks. Extending the interval beyond 8 weeks has not been shown to provide additional benefit.
Myocarditis is inflammation of the heart muscle.
Pericarditis is inflammation of the outer lining of the heart.
· In both cases, the body’s immune system causes inflammation in response to an infection or some other trigger. Learn more about myocarditis and pericarditis. Both myocarditis and pericarditis have the following symptoms:
· Chest pain
· Shortness of breath
· Feelings of having a fast-beating, fluttering, or pounding heart
Myocarditis and pericarditis have rarely been reported. When reported, the cases have especially been in adolescents and young adult males within several days after mRNA COVID-19 vaccination (Pfizer-BioNTech or Moderna). [Emphasis in the original]
· More often after the second dose
· Usually within a week of vaccination
· Most patients with myocarditis or pericarditis who received care responded well to medicine and rest and felt better quickly.
· Patients can usually return to their normal daily activities after their symptoms improve.
· Those who have been diagnosed with myocarditis should consult with their cardiologist (heart doctor) about return to exercise or sports.
Seek medical care if you or your child have any of the specific or general symptoms of myocarditis or pericarditis especially if it’s within a week after COVID-19 vaccination.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/myocarditis.html
Today, the FDA is announcing revisions to the patient and provider fact sheets for the Moderna and Pfizer-BioNTech COVID-19 vaccines regarding the suggested increased risks of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the tissue surrounding the heart) following vaccination. For each vaccine, the Fact Sheet for Healthcare Providers Administering Vaccine (Vaccination Providers) has been revised to include a warning about myocarditis and pericarditis and the Fact Sheet for Recipients and Caregivers has been revised to include information about myocarditis and pericarditis.
...from https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-june-25-2021
The Fact Sheet for Healthcare Providers Administering Vaccine (Vaccination Providers) includes a warning that clinical trial data provide evidence for increased risks of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of tissue surrounding the heart) following administration of Novavax COVID-19 Vaccine, Adjuvanted. The Fact Sheet for Recipients and Caregivers informs that in most people who have had myocarditis or pericarditis after receiving the vaccine, symptoms began within 10 days following vaccination and that vaccine recipients should seek medical attention right away if they experience any of the following symptoms after vaccination: chest pain, shortness of breath, feelings of having a fast-beating, fluttering or pounding heart.
Myth: Children with congenital heart disease are at a higher risk of developing post-vaccine myocarditis.
Fact: "Congenital heart disease is not a risk factor for developing post-vaccine myocarditis. However, it has been identified by the CDC as a risk factor for severe infection for COVID-19."
...Recent data provided by the CDC suggests that among 100,000 vaccinated adolescent males, only about four to seven would be expected to develop post-vaccine myocarditis. If this group was not vaccinated, however, more than 5,500 would be likely to become infected with COVID-19 over a period of three months, with infections resulting in 50 hospitalizations, potential MIS-C, myocarditis and possible death.
...from https://www.chop.edu/news/health-tip/myocarditis-and-covid-19-get-facts
The misinterpretation stems from a comment Gates made during a TED talk in 2010 about methods for reducing the world’s carbon emissions to zero (here). Crucially, one of the factors pushing carbon emissions to an unsustainable level is population growth.
"First, we’ve got population," he said during the talk organized by TED, a non-profit organization devoted to spreading ideas. "The world today has 6.8 billion people. That’s headed up to about nine billion. Now, if we do a really great job on new vaccines, health care, reproductive health services, we could lower that by, perhaps, 10 or 15 percent. But there, we see an increase of about 1.3."
Gates wasn’t talking about decreasing the population -- he was talking about decreasing its rate of growth.
The talk was about reducing global carbon dioxide emissions to zero. It was not describing a plan to use vaccinations to kill people. In fact, his hope for vaccinations is quite the opposite--that good healthcare would lower the risk of death, thereby encouraging parents to have fewer children. This is about slowing the growth of the world population, not reducing the population that exists now.
In an article in Forbes in 2011, Mr Gates said that whilst his initial work in public health focused on contraception, he switched focus to vaccinations, when it became clear that reduced mortality rates and better childhood survival allows individuals to make the choice to reduce their family size, and therefore reduces birth rates.
...from https://fullfact.org/health/viral-video-contains-several-false-pandemic-claims/
Gates is talking about the need to reduce CO2 emissions by humans and he presents this formula for calculating how big these emissions are: CO2 = P x S x E x C (= People x Services per Person x Energy per Service x CO2 per unit of Energy)
It is a mathematical rule that to get something to zero by multiplying you have to multiply it by zero. So, Gates is saying, if you want zero CO2 emissions one of the values on the other side of the equation will have to be zero.
He then goes over them one by one and lists why that wouldn't be practical, ethical or even possible, except maybe with "CO2 per Unit of Energy".
..."If you gave me only one wish for the next 50 years -- I could pick who's president, I could pick a vaccine, which is something I love, or I could pick that this thing that's half the cost with no CO2 gets invented -- this is the wish I would pick."
In other words: Bill Gates would prefer seeing new zero-emission power generation technologies being invented over getting a better and newer vaccine.
So what Gates is saying in his TED talk is almost the opposite of what people using the quote in isolation are claiming. Gates is making the point that reducing the population to zero or even slowing down the growth is not a practical option to stop CO2 emissions and that better power generaton [sic] technology would be a better solution.
This is not academic research.
I'm just googling stuff.
My fact-checking is very basic, not like publications do.
I often have trouble reading scientific studies and the CDC's technical language, so I rely on the media's analysis of scientific data.
Or better yet, meta-analysis of multiple studies.
I also am biased toward dumbed-down stuff.
Sometimes I just link to an article, because I think the answer's there, even though I don't really understand the data.
| ~% of
links on this page... | ...that are from this website: |
| 21% | CDC |
| 6% | YouTube |
| 5% | Wikipedia |
| 3% each | Nature
NY Times |
| 2% each | Vox
Johns Hopkins AP CNN Reuters The Atlantic Forbes Mayo Clinic Media Bias / Fact Check NIH NiemanLab Snopes WHO |
| 1% each | FDA
Business Insider BBC NPR Washington Post medRxiv |
| 35% | ~117 other websites |
(I'm focussing on COVID here, but these principles can be used to fact check anything.)
Contradictory claims can't both be true:
The following are biologically impossible:
The following are logical fallacies / Partial truths / Missing the point:
The CDC has lost all credibility:
If masks work, why does COVID continue to spread?
Masks were useless in the 1918 pandemic.
If your vaccine works, why do you care if I'm vaccinated?
I'm not worried about COVID.
Don't live in fear.
The science isn't settled.
Scientific debate has been suppressed.
The same scientists that tell us we came from monkeys are telling us to get vaccinated and stuff:
I'm following the Bible, not science:
God will protect me:
Everyone should do their own research and decide for themselves:
Mainstream media is pushing one narrative:
People get censored for telling the truth:
Stop commenting on my facebook:
COVID-19 is God's judgement on sin:
COVID-19 isn't bad in my area:
COVID-19 is not your enemy, fear is. You will not die one day sooner or one day later than God has planned for you. But he did not create you to live in fear. The Bible says, 'God has not given us a spirit of fear, but of power, and of love, and of a sound mind.' 2 Timothy 1:7.
How big is the study? The more people, the better for statistical analysis.
We need to look at the numbers over the whole course of the pandemic, or even over a single wave of infection, to see things more clearly. A single set of numbers does not show the whole picture.
Conspiracy theorists quote stastistics just like scientists. But they misinterpret the data. Some examples:
99.97% of infected people recover.
Breakthrough infections (post-vaccination)
Why did more vaccinated than unvaccinated people get infected? (Massachusetts, Israel, Vermont)
[Insert highly-credentialed expert here] disagrees with the scientific consensus.
VAERS underreports adverse events.
Consensus is achieved through scholarly communication at conferences, the publication process, replication of reproducible results by others, scholarly debate,[2][3][4][5] and peer review.
The scientific consensus is based on data.
New data can change the scientific consensus.
The scientific consensus recommends vaccination, masking, social distancing and ventilation.
Public opinion has been slow to adopt the scientific consensus on COVID.
The scientific consensus carries more weight than minority, personal or public opinion.
[Insert highly-credentialed expert here] disagrees with the scientific consensus.
Yes, we are human just like you and we like some things and dislike others. Like you, we want the things we think we see and the easy solutions to be true. Sometimes they are not. In order to prevent bias, MBFC relies 100% on consensus science. In other words, there may be outlying studies that prove differently than the consensus, but we have to abide by the consensus until the consensus changes. For example, GMOs are deadly? There is zero evidence of this. When there is enough evidence to support that claim we will change too and publish accordingly. We do not want to be poisoned or die either. We are opposed to false information for any benefit! Regarding Climate Change, the consensus is it is occurring and influenced by humans... until the consensus tilts otherwise we have no choice but to draw our line and be factual. Sorry. If you consider science to be affiliated with a political party that is sad and we hope to help you navigate through that.
...from https://mediabiasfactcheck.com/frequently-asked-questions/
Media Bias / Fact Check Browser extensions add source rating labels to Google, Facebook, Twitter, Reddit and DuckDuck Go searches.
If you can't find any factually-reliable websites, try well-known websites.
Well-known sources are more likely to have been fact checked or peer reviewed.
Lesser-known sources can get away with more misinformation, because they aren't on the fact checkers' radar.
Only use unknown or unrated websites if you can't find info at factually-reliable or well-known websites.
Things that didn't happen are often poorly documented.
If you can't find any info from factually-reliable or well-known websites, the claim may be made up.
If you google, "Is covid worse in us than other countries?"...
A better search may be "covid deaths statistics".
...The search results will say that COVID-19 is worse in the US than in other countries.
Also essential is understanding our own biases -- what we wish to be true, and how that plays into our decision making.
Every time you search something, it tells the algorithm you’re interested. As you keep searching, you get more of the same. That's how misinformation campaigns get rooted -- a search for a conspiracy theory brings up all kinds of links, which teaches the algorithm that this is what you want. If you want to evaluate a claim, she says, or the person making the claim, do your research in your browser's private or "incognito" mode.
In Chrome, right-click or long press on the image and select "Search Google for image".
In Edge, right-click or long press on the image and select "Search the web for image".
Articles should be based on reliable, independent, published sources with a reputation for fact-checking and accuracy.
I read / watch news every day from these two aggregators:
https://news.google.com/topstories?hl=en-US&gl=US&ceid=US%3Aen
https://digg.com/latest
Providing sources:
Many facebook posts don't provide sources.
Things that didn't happen are often poorly documented.
Readers must be able to check that any of the information within Wikipedia articles is not just made up. This means all material must be attributable to reliable, published sources.
...from https://en.wikipedia.org/wiki/Wikipedia:Verifiability
Two ways to determine source reliability are bias and failed fact checks.
Failed fact checks are more important than bias.
What happened is more important than who said it.
Political leaning is not a factor. The Iffy index includes only sites with low MBFC Factual Reporting levels, which "means the source rarely uses credible sources and is simply not trustworthy for reliable information."
...from https://iffy.news/index/
mediabiasfactcheck.com
NewsGuard
allsides.com
Wikipedia
(Media Bias/Fact Check and Wikipedia often reject a literal interpretation of the Bible.)
All encyclopedic content on Wikipedia must be written from a neutral point of view (NPOV), which means representing fairly, proportionately, and, as far as possible, without editorial bias, all the significant views that have been published by reliable sources on a topic.
LEFT-CENTER BIAS
These media sources have a slight to moderate liberal bias. They often publish factual information that utilizes loaded words (wording that attempts to influence an audience by using appeal to emotion or stereotypes) to favor liberal causes. These sources are generally trustworthy for information, but may require further investigation.
...Factual Reporting: MOSTLY FACTUAL
It really comes down to public trust. And, unfortunately, when political leaders make a political issue out of simple biology, which is that the virus is deadly and the vaccines protect people, it unfortunately deters people from getting vaccinated.
Press releases are just as much about getting attention for the institution, the company, or the researcher, as they are about the research, says Janet Stemwedel, a philosophy professor at San José State University who has written on the topic of evaluating claims in research.
Editorial commentary, analysis and opinion pieces, whether written by the editors of the publication (editorials) or outside authors (op-eds) are reliable primary sources for statements attributed to that editor or author, but are rarely reliable for statements of fact.
...When taking information from opinion content, the identity of the author may help determine reliability. The opinions of specialists and recognized experts are more likely to be reliable and to reflect a significant viewpoint.
...from https://en.wikipedia.org/wiki/Wikipedia:Reliable_sources#News_organizations
Studies at medRxiv haven't been peer reviewed.
Much of mainstream media is left-center biased.
You can check sources for bias here.
Known sources are more likely to be fact checked or peer reviewed.
Mainstream media reports scientific studies.
Science isn't biased.
The CDC is the best information source.
Information sources need evaluated.
Lesser-known sources can get away with more misinformation, because they aren't on the fact checker's radar.
What has changed since April?
Some stuff has changed, but the basics remain the same.
Stuff we still don't know
I view COVID-19 news daily.
And I update this page regularly.
Hopefully my sources do the same.
"What we know so far"
Some stuff has changed, but the basics remain the same.
The Trump administration undermined the CDC.
The CDC is still the best information source.
What has the CDC flip-flopped on?
Centers for Disease Control and Prevention (CDC)
...Bias Rating: PRO-SCIENCE
Factual Reporting: VERY HIGH
...from https://mediabiasfactcheck.com/centers-disease-control-prevention-cdc/
Why are public health officials so bad at talking to us?
...from https://www.vox.com/coronavirus-covid19/22870268/cdc-covid-19-guidelines-isolation-boosters-masks
One problem is, the CDC usually functions more like an academic institution, excelling at producing detailed reports months after an outbreak or episode. It wasn't built to provide real-time analyses or communicate complicated, fast-moving science to the public.
...While there's a limit to how quickly any agency can process the deluge of data created by Covid-19, these experts highlighted the need to improve communication, specifically. "For the longest time, the federal government has treated science communication as an afterthought," Rivera said.
...from https://newrepublic.com/article/165827/cdc-communication-face-masks-walensky-risk
CDC Director Rochelle Walensky is reorganizing the agency, saying it didn't react quickly enough during the Covid pandemic, according an internal review of the agency's operations released on Wednesday.
...Walensky launched the review in April after the massive winter surge of infections from the omicron variant upended the nation's public health response.
...The organizational changes are focused on sharing data more quickly and making public health guidance easier for people to understand.
...from https://www.cnbc.com/2022/08/17/cdc-admits-covid-response-fell-short-launches-reorganization.html
The CDC restructuring follows two reviews conducted in recent months, one by Health Resources and Services Administration official Jim Macrae into the CDC’s pandemic response and another by CDC Chief of Staff Sherri Berger into agency operations.
The reviews concluded that the “traditional scientific and communication processes were not adequate to effectively respond to a crisis the size and scope of the COVID-19 pandemic,” according to an agency statement.
Specifically, Macrae’s review, which included 120 interviews with CDC staffers and people outside the agency, recommended a series of improvements, including releasing scientific findings and data more quickly to improve transparency, translating science into practical and easy-to-understand policy, improving communication with the public, working better with other agencies and public health partners, and training and incentivizing the agency’s workforce to respond better to public health emergencies.
...from https://www.politico.com/news/2022/08/17/cdc-agency-overhaul-covid-19-response-00052384
DATE: March 10, 2021
TO: Rochelle P. Walensky, MD, MPH
Director, CDC, and Administrator, ATSDR
FROM: Anne Schuchat, MD (RADM, USPHS, Ret.)
Principal Deputy Director, CDC
SUBJECT: Summary of Guidance Review
BACKGROUND:
As part of your pledge to lead an effort to restore the public's trust in the CDC, you asked me to begin a comprehensive review to ensure that all of CDC's existing guidance related to COVID-19 is evidence-based and free of politics.
...General observations: [emphasis in the original] There were a variety of issues identified including a) guidance that was not primarily authored by CDC staff; b) reliance on less directive language (e.g., 'considerations') than response leadership felt could be supported by existing evidence; and c) availability of new data or evolving scientific understanding that necessitated updated recommendations.
...Guidance removed: [emphasis in the original] By the time of my review in late January and February 2021, two documents developed or finalized outside of the agency had already been removed ("The Importance of Reopening of America's Schools this Fall" posted July 23, 2020 -- removed October 29, 2020) or replaced (Overview of Testing for SARS-COV-2 posted August 24, 2020, replaced September 18, 2020). A link to a third document ("Opening up America Again" which was released on April 16, 2020 through a link posted on CDC's web) was removed February 7, 2021 during the process of my review (Table 1).
...from PDF (pp 1-2) at https://www.cdc.gov/coronavirus/2019-ncov/downloads/communication/Guidance-Review.pdf
I like making an important point about authorities and false authorities -- credentials actually don't matter, but what does matter is evidence. And we want high quantity and quality of said evidence, something absolutely missing from the claims that Doshi makes.
However, there are substantial reasons why credentials can matter. They imply many things -- a broad education in the science of the subject matter, hard work in the minutiae of that field of science, and approval by one's peers. Getting a Ph.D. in epidemiology is not simply taking classes, but it's actually doing research in the laboratory and field with a published thesis that is reviewed by numerous peer-scientists.
From an opinion of physicians around the country--many of them, maybe all of them, are really well-meaning and quite competent--They're doing that. But they're doing it on the hunch that it will work and be safe. When you get a formal recommendation from a regulatory agency, or a public health agency--like the FDA and the CDC respectively--that will be based on data that's accumulated. We're not there yet--That doesn't mean it's not gonna ultimately happen--but the data don't show that right now.
Evaluating claims is better than evaluating sources.
Citing failed fact checks is better than saying a source has been wrong.
Pew Research
factcheck.org
Full Fact
Australian Associated Press
Lead Stories
AFP
Politifact
Duke Reporters' Lab
Ballotpedia
Wikipedia
Reuters
Snopes
Poynter Institute
Associated Press
USA Today
BBC
CNN
New York Times
Washington Post
Newsweek
As the U.S. reopens a debate into the origins of the novel coronavirus, Facebook reversed course Thursday and said that it would no longer remove posts that claim the virus is man-made.
...from https://www.washingtonpost.com/technology/2021/05/27/facebook-covid-man-made/
The high agreement suggests Snopes and PolitiFact have established consistent and reliable fact-checking practices, they said, which “enhances the credibility of fact checkers in the eyes of the public.”
...from https://www.poynter.org/fact-checking/2023/who-fact-checks-the-fact-checkers-research/
By the time a fact check becomes necessary, two lines of evidence have been presented.
The fact check presents a third line of evidence, possibly corroborating the first line of evidence.
Do we really need a fourth line of evidence?
Example news report:
There's a pandemic.
Evidence:
There's a novel coronavirus.
We're immune-naive to it, and it's spreading like crazy.
Excess deaths.
Example conspiracy theory:
There's no pandemic.
Evidence:
Weekly CDC reports say only 6% of COVID deaths do not list any comorbidities.
The Johns Hopkins News-Letter reported the claimed number of COVID deaths is equal to the missing number of heart-related and cancer deaths.
The frail people who died of COVID likely would have lived longer.
Some of the listed comorbidities like pneumonia were caused or exacerbated by COVID, simliar to how diabetes or AIDS cause complications.
Death certificates list primary and secondary causes of death.
Johns Hopkins retracted the cited article.
Heart disease and cancer were underreported early in the pandemic, because people were scared to seek care.
COVID precautions virtually eliminated flu in 2020.
Heart disease, cancer and COVID were the three leading causes of death in the US in 2020 and 2021, respectively.
Excess deaths.
One path to a solution is “adversarial fact-checking.” Fact-checking is often done by teams of two or more journalists rather than by a single person.
The trouble is, fact-checkers have expanded their purview from checking strictly empirical statements to "checking" contestable political statements.
...from https://newrepublic.com/article/156039/political-fact-checkers-distort-truth
Fact checkers also often "check" opinions, rather than factual claims, even though two people can form diametrically opposed opinions based on the same facts.
...from https://www.investors.com/politics/editorials/fact-checkers-big-media/
She said that, at the moment, there is more misinformation posted from right-wing sources than by the left. This is in part due to Trump, she said, as many of his supporters are repeating things he has said that are not supported by evidence and facts.
...from https://www.cnn.com/2020/10/29/tech/fact-checkers-facebook-trump/index.html
A post-2016 innovation, the labels aren't placed by Facebook but by harried subcontractors, fact-checkers and journalists, and scientists who are fed a never-ending feed of potential misinformation.
...In some cases, Facebook may intervene if it thinks that a piece of content was mistakenly rated, by asking fact-checkers to adjust their ratings, a spokesperson acknowledged to Fast Company.
This would seem to break with a policy that says fact-checkers, not Facebook, are responsible for determining the rating on a piece of content, and that publishers must appeal their ratings to the fact-checkers directly.
...Any content is eligible for review, except politicians' posts and opinion content, an exemption designed in part to avoid appearing to be an "arbiter of truth"--and more pointedly, to deter persistent allegations of anti-right-wing censorship. (Those allegations remain as loud as ever, notwithstanding a lack of evidence that Facebook perpetrates systematic bias against conservatives, and despite Facebook's own data showing that right-wing content is consistently the platform's most engaging.)
There's bias in the training data that the automated content moderation algorithms are trained on. The algorithms that automated content moderation are also hypersensitive. On top of that the sort of policies that these companies make to police content on their platforms are oftentimes created by a small number of men--often cisgender men, white men--that are at the executive level. Lastly I'd say that the community flagging features are often abused by anti-pornography and anti-queer activists online. And because queer identities are so often sexualized and pornographied they tend to be collateral damage in this war on pornography.
GLAD's 2023 social media safety index called social media platforms "Unsafe" for the LGBTQ community. Digital activist Imran Ahmed adds that the platforms aren't just unsafe--they thrive off the toxicity. "That business is addiction--They need you to spend as much time as possible watching their feed, because that's how they make their money. 98% of the revenue of a company like Meta comes from advertising placed into that feed. And so what they are always trying to do is find the most contentious, the most chewy, the most controversial content, because they've worked out that's the most addictive.
...That's the stuff that keeps you scrolling--keeps you on the platform arguing and shouting at each other, and make sure that's seen by as many people as possible. And that's why we've seen such an increase in the amount of hate and disinformation that we're exposed to on a day-to-day basis--because the platforms amplify it at the expense of tolerance, good information--stuff that might actually be useful for society.
November 13, 2020... It was, they declare, resorting to Trump's sort of dramatic language, "the most secure in American history."
...from https://apnews.com/article/top-officials-elections-most-secure-66f9361084ccbc461e3bbf42861057a5
December 1, 2020... Barr told the AP that U.S. attorneys and FBI agents have been working to follow up specific complaints and information they've received, but "to date, we have not seen fraud on a scale that could have effected a different outcome in the election."
...from https://apnews.com/article/william-barr-no-evidence-election-fraud-b1f1488796c9a98c4b1a9061a6c7f49d
January 6, 2021... I've supported the president's right to use the legal system, dozens of lawsuits, perceived hearings in courtrooms all across our country. But over and over, the courts rejected these claims -- including all-star judges whom the president himself has nominated. [-Mitch McConnell]
January 16, 2021... The campaign lost 64 of 65 lawsuits.
...from https://en.wikipedia.org/wiki/Electoral_fraud#United_States
April 9, 2021... 100 lawsuits, in 15 states and the District of Columbia, have been filed (78 have concluded).
...Two presidential recounts (in Georgia and Wisconsin) have been conducted.
Lawsuits related to the 2020 United States presidential election
MyPillow guy scares off Newsmax anchor by talking about voting machine fraud (YouTube)
One America News has quietly scrubbed its website of references to election conspiracy theories, a possible attempt to fend off a lawsuit from the election technology companies it had targeted in its stories.
"Do not conflate voting system security and SolarWinds," tweeted Krebs, who served as US Cybersecurity and Infrastructure Security Agency Director until late November. "The proof is in the paper. You can audit or recount again to confirm the outcome. Like they did in Georgia. And Michigan. And Wisconsin. And Arizona. Can't hack paper."
...from https://www.businessinsider.com/krebs-do-not-conflate-voting-security-solarwinds-hack-2020-12
December 24, 2020... That transition is still in progress, but paperless machines have been eliminated in Georgia, Michigan, Pennsylvania and Wisconsin -- the states Trump supporters have focused on since November. Wherever paper ballots are used, officials can check behind the machines with recounts and audits to find out whether the software was honest.
While mail ballots are more susceptible to fraud than in-person voting, it is still more likely for an American to be struck by lightning than to commit mail voting fraud.
...from https://www.brennancenter.org/our-work/analysis-opinion/false-narrative-vote-mail-fraud
The lightning statistic above disagrees with the lightning statistic below.
In terms of security, both mail-in and absentee ballots are paper ballots hand-marked by the voter, which the National Conference of State Legislatures considers the "gold standard of election security." Forty-four states have signature verification protocols for mail ballots.
...from https://www.nytimes.com/article/fact-checking-mail-in-voting.html
To create a counterfeit ballot, its' physical parameters would have to be exactly matched, as well as the printing with precise timing marks which control how the ballot is scanned by tabulator machines. To have any impact on a national election, many counterfeit ballots would have to be generated and entered.
...While a physical envelope could be created, the barcode voter ID number must match with the election data base maintained in every jurisdiction. Unless the numbers match, law enforcement would be notified.
...The number of envelopes must match the number of physical ballots that are processed by the tabulators. This would prevent the wholesale entry of non-official ballots into the system. The likelihood of pallets of illegal ballots being entered into the process is virtually non-existent and impossible.
In April 2020, a 20-year voter fraud study by MIT University found the level of fraud "exceedingly rare" since it occurs only in "0.00006 percent" of instances nationally, and, in one state, "0.000004 percent--about five times less likely than getting hit by lightning in the United States.[99]
Trump's long White House campaign against verifiable reality has culminated with his lie that he is the true winner of the 2020 presidential election he clearly, certifiably and fairly lost.
To many of us, it's ludicrous nonsense. But to millions of deluded Americans, it's the truth. And it has now gotten people killed.
...from https://www.cnn.com/2021/01/16/politics/fact-check-dale-top-15-donald-trump-lies/index.html
...from https://www.politico.com/news/magazine/2022/03/30/covid-parachute-risk-adaptive-recovery-00021496
There's no silver bullet.
Washing hands and not touching your face eliminates the risk of surface transmission, unless you're licking stuff.
Multiple imperfect precautions work together. (YouTube)
Ventilation clears the air of the virus.
Masking filters out virus that is in the air.
Social distancing isolates you from the virus.
Vaccination reduces risk if you are exposed to the virus.
4 Tips to Keep Your Glasses from Fogging Up (YouTube)
If your mask has a nose wire, pinch it before and/or after donning your mask to make a tighter fit. (YouTube)
Adam Savage used Graf Lanz cloth masks with glasses.
Prioritize bathrooms.
Clean something daily or weekly instead of cleaning everything at once.
Don't de-clutter while you're cleaning.
Or, de-clutter to make it easier to clean.
Reward yourself when you're done.
Ventilation clears the air of the virus.
Masking filters out virus that is in the air.
Social distancing isolates you from the virus.
Vaccination reduces risk if you are exposed to the virus.
Not knowing stuff is exhausting.
We're faced with a lot of the same decisions from our pre-corona lives -- except now, even the most mundane activities have turned into moral dilemmas. Whether it's trying to decide if you should visit a sick family member, order delivery, take public transit, or take a trip to the grocery store, we now have to think through the potential implications of many of our totally normal, everyday actions and decisions in a way we never had to before, because of how they could affect others. This is called "moral fatigue," and it's exhausting.
Well, everyone should understand that this virus is not going away. It's going to be with us for a long time.
So, any hope that you can sort of sit it out and ride out the storm is an unrealistic one, again, another reason why it's great to arm yourself against the virus, your first contact with the virus, through vaccines.
Although it is not clear how strong or long-lasting that immunity will be, especially from Omicron, Americans may slowly be developing the protection from past bouts with Covid that other countries generated through vaccinations -- at the cost, scientists said, of many thousands of American lives.
...from https://www.nytimes.com/interactive/2022/02/01/science/covid-deaths-united-states.html
How is herd immunity achieved?
There are two main paths to herd immunity for COVID-19 -- infection and vaccines.
Natural infection
Herd immunity can be reached when enough people in the population have recovered from a disease and have developed protective antibodies against future infection.
However, there are some major problems with relying on community infection to create herd immunity to the virus that causes COVID-19:
· Reinfection. It's not clear how long you are protected from getting sick again after recovering from COVID-19. Even if you have antibodies, it's possible that you could get COVID-19 again.
· Health impact. Experts estimate that in the U.S., 70% of the population -- more than 200 million people -- would have to recover from COVID-19 to halt the pandemic. This number of infections could lead to serious complications and millions of deaths, especially among older people and those who have existing health conditions. The health care system could quickly become overwhelmed.
Vaccines
Herd immunity also can be reached when enough people have been vaccinated against a disease and have developed protective antibodies against future infection. Unlike the natural infection method, vaccines create immunity without causing illness or resulting complications. Using the concept of herd immunity, vaccines have successfully controlled contagious diseases such as smallpox, polio, diphtheria, rubella and many others.
Herd immunity against COVID-19 should be achieved by protecting people through vaccination, not by exposing them to the pathogen that causes the disease.
The IHME model estimates a wide range -- from 63% to 81% of Americans.
...The omicron wave that assaulted the United States this winter also bolstered its defenses, leaving enough protection against the coronavirus that future spikes will likely require much less -- if any -- dramatic disruption to society.
And although scientists can estimate herd-immunity thresholds, they won't know the actual numbers in real time, says Caitlin Rivers, an epidemiologist at the Johns Hopkins Center for Health Security in Baltimore. Instead, herd immunity is something that can be observed with certainty only by analysing the data in retrospect, maybe as long as ten years afterwards, she says.
May 2, 2021... But herd immunity is slipping away because a quarter of Americans are refusing to get the COVID-19 vaccine. "There is no eradication at this point, it's off the table," Dr. Gregory Poland, director of the Mayo Clinic's Vaccine Research Group, recently said. "We as a society have rejected" herd immunity.
Hmm, no! "We" have not rejected anything. A quarter of the country is ruining it for all of us.
...from https://news.yahoo.com/time-start-shunning-vaccine-hesitant-080043779.html#
Rather than the much-discussed "herd immunity," the morbidity levels being back to nearly normal shows "herd safety," he said.
"This spring, so many people walking around had a recent immune-generating event, vaccine, booster, or infection," with 80% of the Massachusetts population being fully vaccinated, he added. "So now we have something to show for that, but we don't know how long it will last."
...from https://www.medpagetoday.com/infectiousdisease/covid19vaccine/100351
Cases in the U.S. started declining when about 40% of the population was vaccinated with at least one dose, which happened around April 14, said Monica Gandhi, an infectious diseases specialist at the University of California, San Francisco. Infectious diseases experts call this moment the inflection point -- when there was enough immunity in the population to change the tide of the pandemic.
Israel saw an inflection point early March, when 40% of the adult population became fully vaccinated. After the inflection points in Israel and the U.S., cases have steadily declined day after day, week after week.
...from https://www.huffpost.com/entry/examples-covid-19-vaccines-working_l_60b63be1e4b0f2a82eeea4f0
Leading causes of death, US, 2021, provisional
5 Leading causes of death, By age, US, March 2020 - October 2021
Different views on lockdowns
"After pointing out, correctly, the indirect damage caused by the pandemic, they respond that the answer is to increase the direct damage caused by it"
The intensity of the sudden stop induced by the COVID-19 outbreak produces effects which are similar to those of a large-scale, extreme, natural disaster (6–11).
This is why it’s important to distinguish between “short-term lockdowns with underlying goals” and “long-term lockdowns that hope to beat the odds and keep Covid out indefinitely,” said Miller. Brief lockdowns that helped “flatten the curve” were effective and helped keep hospitalizations and deaths down. But extended lockdowns, like the ones seen in China, failed to contain the virus and damaged the country’s economy and well-being.
Research suggests the pandemic's social, economic, and healthcare system disruptions precipitated excess deaths through a variety of mechanisms. Drug overdoses spiked, homicides soared. Patients and providers postponed preventive health and cancer screenings. Medical care diverted to COVID-19 patients delayed treatment of acute conditions such as heart attacks and strokes. Though road traffic decreased during stay-at-home orders in 2020, certain risky behaviors such as driving under the influence and speeding increased among some groups.
...from https://www.medpagetoday.com/opinion/second-opinions/100388
Arguments for the proposition that the “cure is worse than the disease” and the key counter arguments
| Health domain | Argument | Key counterarguments |
| Short-term mortality | Lockdowns themselves caused an increase in short-term excess mortality (defined as mortality greater than the anticipated modelled number of deaths given existing trends) | Countries that imposed several strict lockdowns without experiencing large COVID-19 epidemics (eg, Australia, New Zealand) did not have large numbers of excess deaths. This provides strong evidence that lockdowns themselves are not sufficient to cause surges in deaths |
| Disruption to health services | Lockdowns are directly responsible for reduced access to and use of healthcare services, which in turn causes harms to health in the long term | The association between large outbreaks of COVID-19, government interventions and reduced use of non-COVID health services is well established. However, this association may be due to healthcare services being redirected to handle COVID-19 cases or other impacts of the pandemic itself rather than by lockdowns. In addition, there is evidence that people fear becoming infected by SARS-CoV-2 in healthcare settings and thus stay home rather than attend health services |
| Suicide and mental health | Lockdowns have driven increases in the suicide rate | There is consistent and robust evidence from many countries that government interventions to control COVID-19 have not been associated with increased deaths from suicide |
| Global health programmes | Lockdowns have disrupted services for HIV, TB, malaria and vaccination programmes | Such service disruptions are well documented, but the evidence shows that these have been caused by multiple complex direct and indirect consequences of COVID-19, not just stay-at-home orders |
One lesson that Klimek takes from lockdown studies is that there was an early window of opportunity when the virus could have been eliminated — as it was, in effect, in countries such as China, Australia and New Zealand. Had harsher measures been adopted sooner, and more widely, the pandemic might have played out very differently.
...Most scientists agree that lockdowns did curb COVID-19 deaths and that governments had little option but to restrict people’s social contacts in early 2020, to stem SARS-CoV-2’s spread and avert the collapse of health-care systems. “We needed to buy ourselves some time,” says Lauren Meyers, a biological data scientist at the University of Texas at Austin.
...And lockdown policies did bring costs. Although they delayed outbreaks, saving lives by allowing countries to hang on for vaccines and drugs, they also brought significant social isolation and associated mental-health problems, rising rates of domestic violence and violence against women, cancelled medical appointments and disruption to education for children and university students. And they were often (although not always) accompanied by economic downturns.
Enforcement of Zero-Covid, in the absence of targeted and sufficient vaccination and boosting of the elderly and others, creates higher—not lower—danger for vulnerable populations. Having hundreds of thousands of health workers presently dedicated to testing, isolation, and quarantine leaves far fewer staff available to accelerate vaccinations. The refusal on nationalist grounds to move strategically on introducing Western mRNA vaccines and antivirals at scale (combined with China’s failure thus far to develop its own mRNA vaccines and effective antivirals) means that closing China’s immunity gap is being unnecessarily delayed.
...from https://www.csis.org/analysis/chinas-zero-covid-what-should-west-do
We don't know who's sick. (YouTube)
How many cases are asymptomatic?
We don't know who's sick. (YouTube)
How many cases are asymptomatic?
Respecting the needs of immunocompromised people isn't about disproportionately accommodating some tiny minority; it's really about empathizing with your future self. "Everyone's going to deal with illness at some point in their life," Levantovskaya said. "Don't you want a better world for yourself when that time comes?"
For example, if someone with measles is surrounded by people who are vaccinated against measles, the disease cannot easily be passed on to anyone, and it will quickly disappear again. This is called 'herd immunity', 'community immunity' or 'herd protection', and it gives protection to vulnerable people such as newborn babies, elderly people and those who are too sick to be vaccinated.
But as soon as you try to figure out exactly how it would work, you quickly see that it is actually a remarkably efficient way to kill an unthinkable number of people, which is why Britain, which had initially considered using essentially this strategy, soon abandoned the idea, and moved to the same strategy as the rest of the world: try to reduce transmission until the disease can be controlled by testing and spot-quarantines, rather than national lockdowns. There is no easy way out of this, no simple solution that somehow eluded the experts. There is only a miserable tradeoff between economic production and human lives.
New data from the Zoe symptom-tracker app suggests one in two people with new coldlike symptoms will have COVID-19 rather than the common cold.
Tim Spector, an epidemiologist and the study's lead author, said in a press release on Thursday that for most people, getting infected with Omicron would feel "much more like the common cold, starting with a sore throat, runny nose and a headache," rather than fevers, continuous cough, or loss of taste or smell.
Experts have warned that we can't tell Omicron's severity from the early data we have.
...from https://www.businessinsider.com/is-omicron-severe-covid-hospitalization-rate-severity-2021-12
"The common cold is generally not lethal, with some rare exceptions", the Digital Health Lab explains. "The flu, which is deadlier than the common cold, killed 0.1% of the people who contracted it in 2019. It is still too early to discern accurate global death estimates for people who have contracted COVID-19, but estimates have ranged from 1% to 25% of all cases, depending on the country".
The experts argue that a conservative death rate of 1% would therefore make COVID-19 at least 10 times as deadly as the flu, and therefore "significantly more lethal" than the common cold.
These early studies indicated that COVID-19 illness caused by Omicron tended to be milder than Delta in relatively young populations with high levels of immunity, whether from vaccination or prior infection. But experts said that the data can't tell us if the virus is inherently less deadly than Delta, while others warned Omicron's transmissibility may pose the biggest threat.
...For example, if it takes longer for people with Omicron to need hospital treatment than those with Delta, the results will be an "underestimate," the researchers said in the briefing.
...from https://www.businessinsider.com/is-omicron-severe-covid-hospitalization-rate-severity-2021-12
However, laboratory studies have also shown changes in how Omicron infects our bodies. It is better at infecting our airways rather than the deep tissues of the lungs - this could make it easier for the variant to spread, but milder as it is further away from the delicate parts of the lungs.
...However, a milder virus could still put pressure on hospitals because it spreads so fast.
The issue remains that any benefit of a milder virus could be wiped out by large numbers of people catching Omicron.
..."Vaccination remains vital to protect against severe disease and also to protect against future variants."
William Hanage, epidemiologist at the Harvard T.H. Chan School of Public Health, told The New York Times that the new findings showed unvaccinated people who hadn't yet caught COVID-19 were at "especially high risk."
"If you are unvaccinated and you have never been infected, it is a little less severe than Delta," Dr. Hanage said about the findings, per the Times. "But that's a bit like saying you're being hit over the head with one hammer instead of two hammers. And the hammers are more likely to hit you now," he added.
...from https://www.businessinsider.com/is-omicron-severe-covid-hospitalization-rate-severity-2021-12
Complicating the country’s understanding of this BA.5 wave is a dearth of data. Not since the earliest months of the pandemic has there been so little precise information about the number of actual infections in the United States. As public testing sites have closed and at-home testing — if people test at all — has grown common, the publicly reported data has become scarce and spotty.
...from https://www.nytimes.com/2022/07/18/us/covid-us-outlook.html
While CDC strives to provide complete and accurate data, there are a few challenges. First, COVID-19 can cause mild illness, and symptoms might not appear immediately. This can lead to delays in testing and reporting. Also, not every infected person will get tested or seek medical care, especially if symptoms are not present. Finally, there are differences in how states and territories report cases. The number of new cases reported each day can fluctuate, and reporting frequency can vary by jurisdiction. Health departments may also update case data over time as they receive more complete information.
For these reasons, there might be discrepancies between numbers reported by CDC versus by health departments. When this occurs, data reported by health departments should be considered the most accurate.
CDC estimates that from February 2020--September 2021:
1 in 4.0 (95% UI* 3.4 -- 4.7) COVID--19 infections were reported.
1 in 3.4 (95% UI* 3.0 -- 3.8) COVID--19 symptomatic illnesses were reported.
1 in 1.9 (95% UI* 1.7 -- 2.1) COVID--19 hospitalizations were reported.
1 in 1.32 (95% UI* 1.29 -- 1.34) COVID-19 deaths were reported.
...from https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burden.html
Raw numbers of deaths from all causes compared to previous years, United States
CDC: Excess deaths dashboards
In times of upheaval --wars, natural disasters, outbreaks of disease --researchers need to tally deaths rapidly, and usually turn to a blunt but reliable metric: excess mortality.
Excess deaths are typically defined as the difference between the observed numbers of deaths in specific time periods and expected numbers of deaths in the same time periods.
...from https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm
The study authors noted that all-cause death data are better measures of the true impact of the pandemic than reported COVID-19 deaths because they are less sensitive to coding errors, competing risks, and possible misclassifications in the cause of death; as such, they facilitate comparisons between countries.
...from https://www.cidrap.umn.edu/news-perspective/2021/11/pandemic-marked-premature-deaths-lost-years-life
...2010-2019 data from https://www.snopes.com/tachyon/2021/01/Screen-Shot-2021-01-05-at-3.11.31-PM.png (image)
...from https://www.snopes.com/fact-check/typical-year-covid-deaths/
...from
Countries have reported some five million COVID-19 deaths in two years, but global excess deaths are estimated at double or even quadruple that figure.
...The Economist magazine in London has used a machine-learning approach to produce an estimate of 12 million to 22 million excess deaths -- or between 2 and 4 times the pandemic's official toll so far (see go.nature.com/3qjtyge and 'Global toll').
...The 116 countries and territories in the World Mortality Dataset have reported 4.1 million COVID-19 deaths so far, but their combined excess mortality is around 1.6 times higher, at 6.5 million.
Our approach to estimating the total COVID-19 death rate is based on measurement of the excess death rate during the pandemic week by week compared to what would have been expected based on past trends and seasonality. However, the excess death rate does not equal the total COVID-19 death rate. Excess mortality is influenced by six drivers of all-cause mortality that relate to the pandemic and the social distancing mandates that came with the pandemic. These six drivers are: a) the total COVID-19 death rate, that is, all deaths directly related to COVID-19 infection; b) the increase in mortality due to needed health care being delayed or deferred during the pandemic; c) the increase in mortality due to increases in mental health disorders including depression, increased alcohol use, and increased opioid use; d) the reduction in mortality due to decreases in injuries because of general reductions in mobility associated with social distancing mandates; e) the reductions in mortality due to reduced transmission of other viruses, most notably influenza, respiratory syncytial virus, and measles; and f) the reductions in mortality due to some chronic conditions, such as cardiovascular disease and chronic respiratory disease, that occur when frail individuals who would have died from these conditions died earlier from COVID-19 instead. To correctly estimate the total COVID-19 mortality, we need to take into account all six of these drivers of change in mortality that have happened since the onset of the pandemic.
Viral posts wrongly suggest that the COVID-19 death toll is exaggerated because “the state” has instructed that “anyone who didnt die by a gun shot wound or car accident” be listed as a coronavirus victim. Experts say there is no such default classification — and that the U.S. death count is probably underestimated.
...from https://www.factcheck.org/2020/04/social-media-posts-make-baseless-claim-on-covid-19-death-toll/
Are people who have died in car accidents counted as COVID-19 deaths?
...The Verify team started with a simple Google search.
We found two articles from this year which say that a person who was in a motor vehicle crash was counted as a COVID-19 death. We reached out to health officials in those cases to find out what happened.
In Berks County, Pennsylvania, a local news station reported that a man who was hospitalized after a car accident died of COVID-19.
So what really happened?
We contacted the county coroner, Jonn M. Hollenbach, D-ABMDI, to get more details on the incident. Hollenbach told us first responders were told the man had a coughing spell which caused him to lose consciousness and crash. On the county death certificate, the man's death is labeled as virus-related respiratory failure.
Hollenbach explained further that while the coughing fit happened inside a car, it wasn't the injuries from the car-crash that resulted in his death.
“In this case, the man did not have any life-threatening injuries as a result of the crash," Hollenbach told Verify researchers in an email. "He was tested for COVID-19 upon admission to the hospital due to his symptoms. There was never any report that the crash caused his death."
This past July, Fox 35 Orlando reported that "a person who died in a motorcycle accident was added to Florida’s COVID-19 death count." In an updated story, they say their investigation led to another investigation, and that the death was ultimately removed from the county's COVID-19 death totals.
· In 2019, 629,898 people in the U.S. received an abortion. This equals 11.4 abortions per 1,000 women aged 15--44 years or 191 abortions per 1,000 live births.
· This is an underestimate; the true number of abortions in the United States is closer to 1.2 million a year.
...from https://yourlocalepidemiologist.substack.com/p/banning-abortions-will-not-stop-abortions
(US)... 2017-2018 season... flu... 52,000 deaths (est.)
...from https://www.cdc.gov/flu/about/burden/2017-2018.htm
The number of cases of flu-related illness that occurred during 2017-2018 was the highest since the 2009 H1N1 pandemic, when an estimated 60 million people were sick with flu (2).
I'm not scared of dying at the moment.
I'm scared of killing someone else.
September 16, 2022... Kids are at increased risk for respiratory diseases this flu season.
September 6, 2022... Flu season has only just begun, but some health officials are warning that this year it may start sooner and be more severe.
This prediction comes from looking at Australia, where flu season is now coming to an end.
"We inform what we see in our flu season mainly by Australia and New Zealand-- in the other part of the world where seasons are flipped," explains Dr. Joshua Lenchus, Chief Medical Officer at Broward Health. "What they are seeing there are higher incidents of flu than we have seen in years prior."
In fact, data shows Australia has had its worst flu season in five years.
According to the Australian Department of Health's annual Flu Surveillance Report, in 2021, there were only three patients hospitalized due to flu and no deaths.
This year, however, there have already been 1,708 hospital admissions and 288 deaths.
January 18, 2022... The flu hospitalization rate is still about half of the pre-Covid normal, but it is eight times higher than it was last year when one side effect of pandemic restrictions was that flu cases fell off dramatically.
...from https://www.vox.com/coronavirus-covid19/22878202/us-covid-19-flu-cases-hospitals-vaccines
November 20, 2020... Although we think of the flu as highly contagious given how many of us catch it, it seems to be the case that we have never bothered trying to not spread it around in the past. It is in fact much less contagious than the novel coronavirus, and the measures we have in place to deal with the latter are effectively stamping out the former.
...from https://www.ft.com/content/879f2a2b-e366-47ac-b67a-8d1326d40b5e
Partly false: The claim that tests can misdiagnose a common cold as COVID-19 are misleading. Swab tests used to diagnose COVID-19 are highly specific, experts say. Antibody tests, however, can establish if someone has antibodies from other coronaviruses, but they are not being used to diagnose COVID-19.
Some newer coronavirus tests can now also simultaneously test whether a patient is positive for influenza, but the CDC’s February 2020 PCR test only has the capacity to detect signs of a COVID-19 infection.
...She said the agency was encouraging labs to switch to tests that can also detect influenza at the same time, since it will "save both time and resources."
...Some posts online falsely said the test was unable to differentiate between coronavirus and influenza, leading to inflated COVID-19 counts and depressed flu counts.
In fact, PCR tests are designed to detect very specific areas of the viral genome, so tests do not get confused between which virus is present, said Matthew Binnicker, director of the clinical virology lab at the Mayo Clinic in Rochester, Minnesota.
"PCR tests, including the one developed by the CDC, are highly accurate and are able to differentiate between SARS-CoV-2 and influenza," Binnicker said. "In other words, a COVID-19 test will not be positive if a person really has influenza, and vice versa."
You cannot tell the difference between flu and COVID-19 just by looking at the symptoms alone because they have some of the same symptoms. That's why testing is needed to tell what the illness is and to confirm a diagnosis. Testing is also important because it can reveal if someone has both the flu and COVID-19 at the same time.
October 22, 2020... The southern hemisphere avoided such an eventuality. Their recently concluded flu season was exceptionally mild. It is possible that behind the apparently low caseload lay thousands of undetected patients. Perhaps influenza testing fell away as countries concentrated their resources on COVID-19. Large numbers of people might have struggled through bouts of influenza at home, hidden from the statisticians. In a briefing to the media on June 15, 2020, WHO director-general Tedros Adhanom Ghebreyesus noted that "influenza surveillance has either been suspended or is declining in many countries, and there has been a sharp decline in sharing of influenza information and viruses because of the COVID-19 pandemic". He added that "compared with the last 3 years, we've seen a dramatic decrease in the number of specimens tested for influenza globally".
...from https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30508-7/fulltext
They argued that public health officials should begin by discarding distinct case and death counts for flu, Covid-19, RSV, and other respiratory illnesses. Instead, they say we should focus on the aggregate risk of all these diseases combined.
...from https://www.vox.com/coronavirus-covid19/22878202/us-covid-19-flu-cases-hospitals-vaccines
On June 11, the CDC implemented its current format that reports COVID-19, pneumonia and influenza-related deaths.
The webpage with provisional deaths includes columns for:
· "Deaths involving Pneumonia, with or without COVID-19, excluding Influenza deaths."
· "Deaths involving COVID-19 and Pneumonia, excluding Influenza."
· "All deaths involving Influenza, with or without COVID-19 or pneumonia" or including COVID-19 or pneumonia.
· "Deaths involving Pneumonia, Influenza or COVID-19."
The variations of pneumonia and influenza deaths are reported alongside COVID-19 deaths because the illnesses exhibit similar symptoms. Considering all three tallies can provide a better understanding of the extent of COVID-19 cases that may have gone undiagnosed.
"Deaths due to COVID-19 may be misclassified as pneumonia or influenza deaths in the absence of positive test results, and pneumonia or influenza may appear on death certificates as a comorbid (when a person has two diseases at once) condition," the CDC's website says. "Additionally, COVID-19 symptoms can be similar to influenza-like illness, thus deaths may be misclassified as influenza."
Despite these new variations, the total provisional count of deaths involving COVID-19 was not significantly reduced. The same goes for confirmed and probable deaths, which continued to increase.
Our ruling: False
Although it's unclear where the Facebook user found the numbers, the CDC did not lower the death count, nor did it admit adding influenza and pneumonia to its COVID-19 death count. The user may have confused the CDC's additional reporting of influenza and pneumonia-related deaths or the fact that the CDC reports two different counts for COVID-19 deaths. We rate this claim FALSE because it is not supported by our research.
The CDC's measure at the root of the claim -- one that looks at pneumonia, influenza and COVID-19 together -- is one that has a public health rationale and that is consistent with past practices, experts told us.
The CDC has for years monitored deaths of pneumonia and influenza together as one measure of the flu's mortality -- as archived CDC pages, such as one from January 2016, show. Influenza can cause pneumonia, and so can the novel coronavirus.
"The PIC category was created as a surveillance indicator to monitor COVID-19 mortality, in the same way that we have used combined pneumonia and influenza deaths, for many years, to monitor influenza mortality," Anderson said. "Pneumonia tends to fluctuate in response to and along with influenza (and COVID-19). This is particularly useful where influenza (or COVID-19) mortality is underreported."
Heart disease and cancer were the two leading causes of US deaths in 2020.
...from https://www.cdc.gov/nchs/products/databriefs/db427.htm
COVID outpaced seven top killers in 2020 (image)
...from
underlying medical conditions that increase a person's risk of severe illness from COVID-19
The institute's study had nothing to do with cancer -- many federal researchers have shifted to coronavirus work because of the pandemic.
Coronavirus vaccinations can cause enlarged lymph nodes in the armpit or near the collarbone, which may be mistaken for a sign of cancer.
...from https://www.nytimes.com/2021/03/01/health/covid-vaccine-lymph-nodes.html#article-summary
Screenings for several major cancers fell significantly during 2020, according to a study published in December 2021 in the journal Cancer. Colonoscopies dropped by nearly half compared to 2019, prostate biopsies by more than 25 percent. New diagnoses declined by 13 percent to 23 percent, depending on the cancer -- not because there was less cancer in the world, but because less of it was being detected.
...from https://www.vox.com/coronavirus-covid19/22841229/covid-19-us-cancer-screenings
April 16, 2020... Further evidence is emerging of dramatic falls in numbers of hospital patients presenting with serious medical conditions such as strokes and heart attacks since the beginning of the coronavirus pandemic.
A US study found that interventions for serious heart attacks have fallen 38% since 1 March. Similar reductions were reported in Spain, while in Lombardy, the worst affected region of Italy, the figure was 70%.
On Wednesday the Guardian revealed that doctors and paramedics in the UK had warned of a sharp rise in the number of seriously ill people dying at home because they were reluctant to call for an ambulance.
Andrew Goddard, the president of the Royal College of Physicians, said: "Consultants in cardiology and emergency medicine are reporting significant reductions in admissions with heart attack symptoms."
Something similar has been happening with stroke. The neurologist David Werring, who chairs the Association of British Neurologists' stroke advisory group, said University College London hospitals NHS foundation trust, where he works, saw a 30% reduction in people being referred with stroke, or treated for stroke, compared with the same period last year.
"There is no reason to assume that the incidence of stroke declined since the onset of the Covid-19 crisis, but in many countries fewer people with symptoms suggestive of stroke present to the hospital," stated the European Stroke Organisation last week, on publishing findings that 80% of stroke care providers across 55 countries were experiencing reduced demand.
"Patients are waiting longer to present with their symptoms," said Goddard.
...Patrik Michel, a neurologist at the Centre Hospitalier Universitaire Vaudois in Lausanne, Switzerland, said that the constraints on indulging in strenuous exercise under lockdown may actually have spared a few people with ailing hearts from a heart attack -- though this is unlikely to have had a major effect on numbers.
Werring said social distancing could similarly be protecting some of those at risk of stroke, because it means that they are less exposed to infections of all kinds. "There's a strong association between infections and stroke," he said.
..."The most important message to patients is that the NHS [UK] is very much open for business as usual for heart attacks and strokes," said Goddard. "The risks of catching Covid-19 are small as the units managing such patients are very distinct from wards looking after Covid-19 patients. The risks of dying from heart diseases or being left with significant long-term effects are much greater."
The increase, or decrease, in the number of detected cases is directly impacted by the number of tests being administered.
...Unless testing of the population is done randomly, the percentage of tested cases that are positive will not reflect the real percentage of the population infected.
...The case fatality rate (CFR), percentage of fatalities in detected cases, is an overestimate of the real infection fatality rate (IFR), and will invariably decrease as testing ramps up.
Case-fatality rates depend on testing: a country that tests only people with severe symptoms, for example, will have an outsized case-fatality rate compared with one in which asymptomatic testing is widespread.
Daily State-by-State Testing Trends
How Coronavirus Cases Compare With Expectations
Track Trends in COVID-19 Cases and Tests
Cases... Tests... Hospitalizations... Outcomes
January 11, 2022... When N95 respirators were in short supply early in the pandemic, the CDC established "crisis capacity" strategies for health care facilities, but noted that this is no longer necessary because respirator supply has increased significantly.
...from https://www.sfchronicle.com/health/article/How-long-can-I-keep-using-the-same-N95-respirator-16765593.php FDA Device Shortage List
Omicron sub-lineage BQ.1.1 is the first variant resistant to all antibody therapies currently approved by the EMA (European Medicines Agency) and/or FDA (US Food and Drug Administration).
...Particularly in regions where BQ.1.1 is widespread, physicians should not rely on antibody therapies alone when treating infected high-risk patients, but should also consider administering other drugs such as paxlovid or molnupiravir,” comments study leader Markus Hoffmann on the results of the study.
...from https://scitechdaily.com/new-covid-subvariant-resistant-to-all-therapeutic-antibodies/
Although the U.S. health care system is among the best in the world, Americans suffer from what experts have called “the U.S. health disadvantage,” an amalgam of influences that erode well-being, Dr. Woolf said.
These include a fragmented, profit-driven health care system; poor diet and a lack of physical activity; and pervasive risk factors such as smoking, widespread access to guns, poverty and pollution. The problems are compounded for marginalized groups by racism and segregation, he added.
The result is a high disease burden among Americans, and shorter life expectancy compared with that in comparable high-income nations over the last two decades, Dr. Woolf said.
...from https://www.nytimes.com/2022/08/31/health/life-expectancy-covid-pandemic.html
In recent months, the United States passed Britain and Belgium to have, among rich nations, the largest share of its population to have died from Covid over the entire pandemic.
...Chief among the reasons is the country's faltering effort to vaccinate its most vulnerable people at the levels achieved by more successful European countries.
...from https://www.nytimes.com/interactive/2022/02/01/science/covid-deaths-united-states.html
A significant proportion of COVID-19 transmission is asymptomatic or presymptomatic -- potentially as high as 60%, according to a 2021 JAMA Network Open modeling study.
...Estimates of asymptomatic disease rates with COVID-19 -- the proportion who are infected but never manifest symptoms -- have ranged from about 25% to 40% throughout the pandemic, with a number of papers, including one in the Annals of Internal Medicine, coming in at about a third of cases.
...from https://www.medpagetoday.com/special-reports/exclusives/98632
Masks are primarily intended to reduce the emission of virus-laden droplets by the wearer ("source control"), which is especially relevant for asymptomatic or presymptomatic infected wearers who feel well and may be unaware of their infectiousness to others (estimated to account for more than 50% of SARS-CoV-2 transmissions).1, 2
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
| Variant: | R0: |
| original | 2.6 (Also, see here) |
| Alpha | 4 |
| Delta | 6.3 (Also, see here) |
| Omicron BA.1 | 9.5 |
| Omicron BA.2 | 6-10? |
| Omicron BA.2.12.1 | ? |
| Omicron BA.5 | 6-10?
(not 18.6) |
| Omicron BQ.1.1 | ? |
| Omicron XBB.1.5 | ? |
A variant can have a growth advantage and not actually be intrinsically more transmissible. In fact, the R0 of variant A may be higher, lower, or the same as variant B.
This is because the growth advantage of variant A, compared to variant B, may be driven by any combination of:
1. a shorter generation time
2. increased intrinsic transmissibility (R0)
3. an increased level of “immune evasion”.
Experts say it would be difficult to accurately calculate the variants’ infectiousness using R0, let alone compare it to other viruses, as the measure is only applicable to populations with no exposure to a virus, and doesn’t account for prior infection or vaccination.
...from https://apnews.com/article/fact-check-r0-measles-covid-variants-infectiousness-423007125020
The 99% isn't the problem. The 1% is.
It's very difficult to estimate mortality risk - when you have something that varies at least by over 1000-fold depending on your age or risk factors, the average is pretty pointless.
...from https://www.ft.com/content/879f2a2b-e366-47ac-b67a-8d1326d40b5e
A person infected with BA.5 may infect 6-10 people.
...Anyone may be contagious.
...Hospitals are overwhelmed with COVID-19...
...20% of infections are severe.
...Long-term effects on infected persons
...Small businesses are struggling.
...and struggle to treat other medical issues.
COVID-19 deaths by age
Anyone may be contagious.
Incidence of COVID cases in kids is comparable to that in adults.
The virus deaths of older people have sometimes been dismissed as losses that might have occurred anyway, from other causes, but analyses of "excess deaths" challenge that suggestion. Eighteen percent more older people died of all causes in 2020 than would have died in an ordinary year, according to data from the C.D.C.
...from https://www.nytimes.com/2021/12/13/us/covid-deaths-elderly-americans.html
Moreover, excluding COVID-19 deaths, Americans in the 65 and older group had lower mortality risks in 2021 than in 2015-2019. This decrease can be explained by mortality displacement: COVID-19 deaths in year 1 of the pandemic for these age groups replaced expected deaths in year 2 from other causes.
...from https://www.medpagetoday.com/opinion/second-opinions/100388
The problem, says Saad Omer, director of the Yale Institute for Global Health, is that many of those deaths in the VAERS database were caused by other illnesses that happened around the same time as the immunization and had nothing to do with a vaccine: "Vaccines decrease your risk of COVID-19," Omer notes. "They don't make you immortal."
In fact, COVID-19 vaccines were given first to some of the oldest and sickest people in America. Their risk of dying from COVID was high, but "their risk of mortality due to other causes was also high. In fact, very high," Omer says.
Unfortunately, the message that covid-19 risk was about the same as the annual risk (and hence that catching the virus roughly doubles the risk of dying this year) was misinterpreted by some as meaning that it did not increase the annual risk at all. In fact, if the risk of dying this year from covid-19 is p, and the risk of independently dying from something else is also p, then probability theory tells us that the overall risk of dying this year is one minus the chance of surviving both hazards--that is, 1-(1-p)(1-p) or 2p-p2. For low p, this will be very close to 2p, and so it is generally fine to say that covid-19 would roughly double the risk of dying. But if you were frail and had a 60% risk of dying next year, then with infection this would rise to 2×0.6--0.62=0.84, so altogether you would have an 84% chance of dying. (The events may also not be independent: survivors may be weakened by the disease or show increased resilience.)
...Importantly, all the risks quoted are the average (mean) risks for people of the relevant age but are not the risks of the average person. This is because, both for covid-19 and in normal circumstances, much of the risk is held by people who are already chronically ill.
...It should always be remembered that these are risks to the individual: there is still a responsibility to consider the potential risks an individual may cause to others.
...Nursing home cases grew by 440% (from 9,000 to 48,800) between July and August 2021, with a slightly higher increase in resident cases (483%, growing from 3,200 to 19,000) than staff cases (416%, growing from 5,700 to 29,600). Cases outside of nursing homes increased by 224% in the same time period, growing from 1.3 million to 4.2 million (Table 1). Similar to COVID-19 deaths, the vast majority of COVID-19 cases occurred outside of nursing homes. However, the high rate of increase of nursing home cases shows the connection between community spread and the spread of the virus in nursing homes.
Yes.
Caregivers likely infected residents. Residents are isolated from the general population, but caregivers are not.
All coronavirus infections start mild, doctors say, and the majority -- about 80% -- stay that way.
COVID-19 cases in schools by state
Schools & Childcare
Incidence of COVID cases in kids is comparable to that in adults.
Immunity wanes following both recovery and vaccination.
So if someone was recently infected with a BA.2 lineage, are they mostly protected against reinfection with BA.4 or BA.5?
Probably not, infectious disease experts say.
...Lawler said it's "quite likely and highly predictable that people who were infected with BA.2 will be susceptible to infection with BA.4 or BA.5, and that susceptibility will grow as time goes on, as you get further away from your prior infection."
...from https://www.medpagetoday.com/special-reports/exclusives/99281
After recovering from COVID-19, most individuals will have some protection from repeat infections. However, reinfections do occur after COVID-19. We are still learning more about these reinfections.
...from https://www.cdc.gov/coronavirus/2019-ncov/your-health/reinfection.html
After a SARS-CoV-2 infection, a person's antibody and T cell responses may be strong enough to provide protection against reinfection. Research shows that 91% of people who develop antibodies against the coronavirus are unlikely to be infected again for six months, even after a mild infection. People who had no symptoms during the infection are also likely to develop immunity, though they tend to make fewer antibodies than those who felt ill.
Available evidence shows that fully vaccinated individuals and those previously infected with SARS-CoV-2 each have a low risk of subsequent infection for at least 6 months. Data are presently insufficient to determine an antibody titer threshold that indicates when an individual is protected from infection. At this time, there is no FDA-authorized or approved test that providers or the public can use to reliably determine whether a person is protected from infection.
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/vaccine-induced-immunity.html
Having a weakened immune system can make you more likely to get severely ill from COVID-19. Many conditions and treatments can cause a person to be immunocompromised or have a weakened immune system. Primary immunodeficiency is caused by genetic defects that can be inherited. Prolonged use of corticosteroids or other immune weakening medicines can lead to secondary or acquired immunodeficiency.
Imprinting was first observed decades ago, in people with influenza. Their immune systems responded to a new circulating strain by producing antibodies tailored to their first flu encounter. In some cases, this led to a poorer ability to fight off the new strain.
The phenomenon can explain some observations from the past, such as the surprisingly high mortality among young adults during the 1918 influenza pandemic. Members of the older generation, exposed in their youth to a flu strain that closely matched the deadly H1N1 pandemic strain, had a more robust immune response than did younger adults, whose first exposure was to a mismatched strain.
With COVID-19, these two arms of the immune system (innate and acquired) obviously work well for 80% of the population who recover from more or less mild influenza-like illness.
In older people, or people with immunodeficiencies, the activation of the acquired immune system may be delayed. This means that the virus can carry on replicating and spreading in the body, causing chaos and damage as it does, but there's another consequence. Another job of the acquired immune system is to stand-down the innate immune system; until that's done the innate immune response will keep increasing as the virus replicates and spreads. Part of the innate immune response is to cause 'inflammation'. That is useful in containing the virus early in an infection but can result in widespread damage of uninfected tissue (we call this a 'bystander effect') if it becomes too large and uncontrolled, a situation named 'cytokine storm' when it was first seen with SARS and avian influenza H5N1. It is difficult to manage clinically, requiring intensive care and treatment and carries with it high risk of death.
Washing hands and not touching your face eliminates the risk from surface transmission.
Unless you're licking stuff.
Findings of these studies suggest that the risk of SARS-CoV-2 infection via the fomite transmission route is low, and generally less than 1 in 10,000, which means that each contact with a contaminated surface has less than a 1 in 10,000 chance of causing an infection 7, 8, 9.
There have been few reports of COVID-19 cases potentially attributed to fomite transmission 1, 2.
...from https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html
December 11, 2020... The coronavirus's genetic material has been found on all kinds of surfaces in hospitals and in the air, but, interestingly, it has only been successfully cultured from the air. No data studies that we are aware of have cultured the virus from surfaces.
...from https://www.washingtonpost.com/opinions/2020/12/11/covid-19-airborne-transmission-cleaning-surfaces/
People can be infected with SARS-CoV-2 through contact with surfaces. However, based on available epidemiological data and studies of environmental transmission factors, surface transmission is not the main route by which SARS-CoV-2 spreads, and the risk is considered to be low. The principal mode by which people are infected with SARS-CoV-2 is through exposure to respiratory droplets carrying infectious virus.
The risk of surface transmission is low.
Washing hands and not touching your face eliminates the risk from surface transmission.
Unless you're licking stuff.
April 5, 2021... Numerous researchers have studied how long SARS-CoV-2 can survive on a variety of porous and non-porous surfaces 10, 11, 12, 13, 14, 15. On porous surfaces, studies report inability to detect viable virus within minutes to hours; on non-porous surfaces, viable virus can be detected for days to weeks. The apparent, relatively faster inactivation of SARS-CoV-2 on porous compared with non-porous surfaces might be attributable to capillary action within pores and faster aerosol droplet evaporation 16.
Data from surface survival studies indicate that a 99% reduction in infectious SARS-CoV-2 and other coronaviruses can be expected under typical indoor environmental conditions within 3 days (72 hours) on common non-porous surfaces like stainless steel, plastic, and glass 10, 11, 12, 13, 15. However, experimental conditions on both porous and non-porous surfaces do not necessarily reflect real-world conditions, such as initial virus amount (e.g., viral load in respiratory droplets) and factors that can remove or degrade the virus, such as ventilation and changing environmental conditions 8, 9.
· The risk of animals spreading COVID-19 to people is low.
· Pets can get serious illness from infection with the virus that causes COVID-19, but this is extremely rare.
...Protect pets if you are sick
If you are sick with COVID-19 (either suspected or confirmed by a test), you should avoid contact with your pets and other animals, just like you would with people. Contact includes petting, snuggling, kissing, licking, sharing food, and sleeping in the same bed.
We already know that the virus can infect and spread within wild mink and white-tailed deer—and for both species, there is at least one verified instance in which the virus has gone from humans to the animals and back again to humans.
...from https://www.nationalgeographic.com/animals/article/how-so-many-animal-species-contract-covid
The cases of COVID transmission from minks and hamsters both happened in situations where people were caretakers for a large number of animals. But just last month, the first evidence of COVID being passed from a cat to a person was reported. According to a study published last month in Emerging Infectious Diseases, the cat sneezed in the face of a veterinary surgeon who was testing the animal for COVID. Three days later the vet tested positive for COVID, but none of the vet's close contacts did, suggesting the vet got the virus from the infected cat.
There's also a concern that wildlife infected with COVID — like a population of deer in Pennsylvania and other parts of North America — could become reservoirs for the virus, meaning the virus can circulate in them, perhaps even mutate into more transmissible or virulent strains and get passed back to humans. "That could mean that there is a continuing risk from those animals for public health," says van der Poel. "But we have not seen [evidence of a wildlife animal reservoir] yet."
Scientists still don't know how those deer got COVID. It's unlikely the deer caught it from direct contact with humans, though transmission from contaminated wastewater or other infected animals, like feral cats, are possibilities.
Do NOT use disinfectants designed for hard surfaces, such as bleach or ammonia, on food packaged in cardboard or plastic wrap.
...Do NOT wash produce with soap, bleach, sanitizer, alcohol, disinfectant or any other chemical.
...The risk of infection by the virus from food products, food packaging, or bags is thought to be very low. Currently, no cases of COVID-19 have been identified where infection was thought to have occurred by touching food, food packaging, or shopping bags.
Currently there is no evidence of food, food containers, or food packaging being associated with transmission of COVID-19.
...from https://www.foxnews.com/world/chinese-ice-cream-contaminated-covid-19
There is no evidence that drinking lots of water flushes out the new coronavirus or the stomach acid kills the virus.
...from (PDF) https://www.who.int/docs/default-source/nepal-documents/novel-coronavirus/un-rumour-tracking-english-issue-2.pdf
And SARS-CoV-2, the virus that causes Covid-19, doesn't seem to hate acid as much as other viruses.
...from https://medium.com/@adrien.burch/can-stomach-acid-kill-coronavirus-b73a2032028f
The amount of time that the air inside an examination room remains potentially infectious is not known and may depend on a number of factors including the size of the room, the number of air changes per hour, how long the patient was in the room, if the patient was coughing or sneezing, and if an aerosol-generating procedure was performed. Facilities will need to consider these factors when deciding when the vacated room can be entered by someone who is not wearing PPE.
...from https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html
When a person with suspected or confirmed COVID-19 has been indoors, virus can remain suspended in the air for minutes to hours. The length of time virus remains suspended and is infectious depends on numerous factors, including viral load in respiratory droplets or in small particles, disturbance of air and surfaces, ventilation, temperature, and humidity 27, 28, 29, 30, 31. Wearing masks consistently and correctly can substantially reduce the amount of virus indoors, including the amount of virus that lands on surfaces 32.
Based on limited epidemiologic and experimental data, the risk of infection from entering a space where a person with COVID-19 has been is low after 24 hours. During the first 24 hours, the risk can be reduced by increasing ventilation and waiting as long as possible before entering the space (at least several hours, based on documented airborne transmission cases), and using personal protective equipment (including any protection needed for the cleaning and disinfection products) to reduce risk.
Handkerchiefs are adequately sanitary if stored away immediately after use (e.g., in a pocket or purse), followed by the user washing his or her hands.
(Exposure risk remains for the person laundering handkerchiefs.)
Tissues are adequately sanitary if disposed of immediately after use, followed by the user washing his or her hands.
(Exposure risk remains for the person removing trash.)
If you are suffering from a cold or the flu, then yes, tissues are a better option. The reason for this is you are essentially blowing nasal secretions containing the virus - that is causing your illness - into the tissue. As long as you throw that tissue into the bin (without re-using) and wash your hands, tissues are the most hygienic option. By using a handkerchief, you are increasing the chance of spreading the virus (not to yourself, as you already have it -- but to those around you). Saliva doesn't contain as much of the virus as nasal secretion, so by blowing your nose several times into a hanky, which is potentially already feeling a little 'damp', you are increasing the spread of virus when touching other items such as door knobs and computer keyboards with your 'hanky hands'.
The risk of surface transmission is low.
Covid virus 'survives for 28 days' in lab conditions
Those questions can be put to bed, experts say, because while the novel coronavirus can survive being frozen, it's highly unlikely to survive in a state that would be able to transmit an infection.
Researchers have demonstrated that SARS-CoV-2 can survive conditions as low as minus 20 degrees Celsius and that the virus thrives in damp, cold conditions. Because the coronavirus can linger on a cold surface, there's a chance humans may become infected by handling products contaminated with viral particles. There's been a moderate incidence of COVID-19 outbreaks in meat packaging facilities in the US, the UK, Germany, Australia and a handful of other nations.
In the case of surgical or N95 masks, sunlight could actually be a bad thing, Flinn said. "We know that prolonged direct sunlight can degrade some of the plastic materials, even the foam in some of our surgical masks," she said. Instructions on a package for a surgical mask sold at a CVS in Potomac, Md., included a similar warning: "Avoid direct exposure of sunlight during storage as the filter media in this mask can be degraded by extended exposure to sunlight."
Higher levels of vitamin D than traditionally considered sufficient may help prevent COVID-19 infection--particularly in Black patients--or lead to less severe outcomes, two new US studies suggest.
Two large clinical trials published by The BMJ today show that boosting vitamin D levels in adults during the SARS-CoV-2 pandemic was not associated with protection against respiratory tract infections or COVID-19.
...The first trial was carried out in the UK between December 2020 and June 2021 and involved 6,200 adults (16 years and over) not using vitamin D supplements at enrollment.
Half (3,100 participants) were offered a vitamin D blood test and those found to have low vitamin D levels (2,674; 86%) received either 3200 IU/day or 800 IU/day of vitamin D supplements for six months, while the other half (controls) received no test or supplements.
...The second trial was conducted in Norway between November 2020 and June 2021 using cod liver oil, which contains low doses of vitamin D and vitamin A as well as omega-3 fatty acids.
A total of 34,741 adults (18-75 years) who were not using vitamin D supplements received either 5 mL cod liver oil or 5 mL placebo (corn oil) daily for six months. The majority of participants (86%) who were tested had adequate vitamin D levels at the start of the study.
...In a linked editorial, Professor Peter Bergman at the Karolinska Institutet in Sweden says vaccination is still the most effective way to protect people from COVID-19, and vitamin D and cod liver oil supplementation should not be offered to healthy people with normal vitamin D levels.
Instead, he suggests clinicians could focus on risk groups, including people with dark skin, or skin that is rarely exposed to the sun, pregnant women, and elderly people with chronic diseases, who could be tested before supplementation.
...from https://medicalxpress.com/news/2022-09-trials-link-vitamin-d-supplements.html
The fascination with vitamin D supplementation began with the discovery in the early 1920s that vitamin D prevented rickets and was further driven by the recognition of other potential roles of vitamin D in non-skeletal outcomes, including immune function, cardiovascular health, and cancer. However, whereas data on the function of vitamin D in bone growth and maintenance is clear-cut and has informed practical clinical guidelines and public health policies over the years, evidence supporting the role of vitamin D in other health and disease processes, in particular in acute respiratory tract infection, remains patchy. Data from observational studies have suggested that vitamin D supplementation can lower the odds of developing respiratory infections, particularly in vitamin D-deficient groups, but randomised trials have yielded mixed results.
...It has long been clear that groups that traditionally exhibit vitamin D deficiency or insufficiency, such as older adults and nursing home residents, and Black, Asian, and minority ethnic populations, are the same groups that have also been disproportionately impacted by COVID-19. Additionally, increased time spent indoors due to strict lockdowns and shielding triggered concerns that some people might not obtain the necessary physiological levels of vitamin D from sunlight.
On Dec 17, 2020, the National Institute for Health and Care Excellence (NICE), in collaboration with Public Health England and the Scientific Advisory Committee on Nutrition, published an updated rapid review of recent studies on vitamin D and COVID-19. Their recommendations support the current government advice, revised in April, 2020, during the first lockdown in the UK, for everyone to take vitamin D supplements to maintain bone and muscle health during the autumn and winter months. The recommendations are also in line with new guidance from the UK government, released on Dec 22, 2020, allowing extremely clinically vulnerable people to opt in to receive a free 4-month supply of daily vitamin D supplements--similar to an initiative launched earlier in Scotland.
Vitamin D toxicity is usually caused by large doses of vitamin D supplements -- not by diet or sun exposure. That's because your body regulates the amount of vitamin D produced by sun exposure, and even fortified foods don't contain large amounts of vitamin D.
...Taking 60,000 international units (IU) a day of vitamin D for several months has been shown to cause toxicity. This level is many times higher than the U.S. Recommended Dietary Allowance (RDA) for most adults of 600 IU of vitamin D a day.
Monitor symptoms.
Use separate bathrooms.
Designate a "sick room" for the infected person to stay in.
Run a humidifier in the infected person's room.
Turn on bathroom exhaust fans.
Isolate pets from infected person.
Ask for help.
...clean more...
...clear the air...
...wash hands more...
...mask...
Free rapid tests... Insurance... Free testing sites
Low or no-cost testing by state
Cost, Place, Insurance
Starting in May, though, beneficiaries in original Medicare and many people with private, job-based insurance will have to start paying out-of-pocket for the rapid antigen test kits.
· The federal program allowing people to order free COVID rapid tests from the government will end on September 2 due to lack of Congressional funding.
· For now, insurance providers must cover up to eight free tests per plan member per month.
· Even without health insurance, there are still several ways to find free or low-cost COVID tests.
...from https://www.verywellhealth.com/low-cost-covid-tests-after-free-white-house-tests-end-6504462
Americans with private insurance will be able to ask for reimbursement for rapid COVID-19 tests beginning Saturday -- but any tests purchased before January 15 will not qualify.
...from https://www.cbsnews.com/news/covid-home-test-insurance-reimbursement-saturday/
When you perform an at-home COVID-19 antigen test, and you get a positive result, the results are typically accurate. However, if you perform an at-home COVID-19 antigen test, you could get a false negative result.
...COVID-19 antigen tests may not detect the SARS-CoV-2 virus early in an infection, meaning testing soon after you were exposed to someone with COVID-19 could lead to a false-negative result, especially if you don't have symptoms. This is the reason why repeat testing is important.
...· If you receive a positive result initially or after a repeat test, this means the test detected the SARS-CoV-2 virus and you most likely have COVID-19.
· Follow the Centers for Disease Control and Prevention (CDC) guidance for people with COVID-19, including to stay home, isolate from others, and seek follow-up care with a health care provider to determine the next steps.
· If you receive a negative result, the test did not detect the SARS-CoV-2 virus at the time of that test.
· If you have COVID-19 symptoms, test again 48 hours after the first negative test, for a total of at least two tests.
· If you get a negative result on the second test and you are concerned that you could have COVID-19, you may choose to test again 48 hours after the second test, consider getting a laboratory molecular-based test, or call your health care provider.
· If you do not have COVID-19 symptoms and believe you have been exposed to COVID-19, test again 48 hours after the first negative test, then 48 hours after the second negative test, for a total of at least three tests.
· If you get a negative result on the second test, test again 48 hours after the second test.
· If you get a negative result on the third test and you are concerned that you could have COVID-19, you may choose to test again using an antigen test, consider getting a laboratory molecular-based test, or call your health care provider.
· If you get a positive result on any repeat test with an at-home COVID-19 antigen test, you most likely have COVID-19 and should follow the CDC guidance for people with COVID-19.
After getting a COVID-19 vaccine, will I test positive for COVID-19 on a viral test?
No. None of the authorized and recommended COVID-19 vaccines cause you to test positive on viral tests, which are used to see if you have a current infection. Neither can any of the COVID-19 vaccines currently in clinical trials in the United States.
If your body develops an immune response to vaccination, which is the goal, you may test positive on some antibody tests. Antibody tests indicate you had a previous infection and that you may have some level of protection against the virus.
...from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/facts.html#
In a world with perfect coronavirus tests, people could swab their nose or spit in a tube and get near-instant answers about their SARS-CoV-2 status. The products would be free, fast, and completely reliable. Positives would immediately shuttle people out of public spaces and, if needed, into treatment; negatives could green-light entry into every store, school, and office, and spring people out of isolation with no second thought. Tests would guarantee whether someone is contagious, or merely infected, or neither. And that status would hold true until each person had the chance to test again.
Unfortunately, that is not the reality we live in--nor will it ever be. "No such test exists," K. C. Coffey, an infectious-disease physician and diagnostics expert at the University of Maryland School of Medicine, told me. Not for this virus, and "not for any disease that I know of."
...from https://www.theatlantic.com/health/archive/2021/11/coronavirus-testing-still-confusing/620783/
The risk of surface transmission is low.
When you're out in public, be aware of surfaces you touch, and wash your hands often. It's much more effective to wash your hands thoroughly than try to clean everything you touch.
By funneling our anxieties into empty cleaning rituals, we lose focus on the more common modes of COVID-19 transmission and the most crucial policies to stop this plague. "My point is not to relax, but rather to focus on what matters and what works," Goldman said. "Masks, social distancing, and moving activities outdoors. That's it. That's how we protect ourselves. That's how we beat this thing."
...from https://www.theatlantic.com/ideas/archive/2020/07/scourge-hygiene-theater/614599/
The best analogy we've used for how this virus is spread is to think about a smoker. If you're near a smoker outside, you may not notice the smell, especially if you're not standing too close. But if you're indoors, you could definitely detect it, even if you're across the room, depending on how far away you are and how well-ventilated or filtered the air is.
How much could you protect yourself from that smoke by scrubbing down countertops, doorknobs and all the other surfaces in the room? Not much. Shared air is the problem, not shared surfaces.
...from https://www.washingtonpost.com/opinions/2020/12/11/covid-19-airborne-transmission-cleaning-surfaces/
DIY Box Fan Air Purifier (YouTube)
Students can even build portable air cleaners themselves. One popular model, the Corsi-Rosenthal box, can be built for under $100. These DIY boxes can perform just as well as expensive air cleaners, says Krystal Pollitt, an epidemiologist and environmental health expert at Yale University. Engineers at 3M, the company which produces the filters commonly used for these boxes, verified that the design is effective.
...from https://time.com/6206343/schools-ventilation-covid-19-air-quality/
They concluded the boxes were effective at capturing unwanted airborne particles, including viruses, (link to results) and serves as a good supplement to a more holistic ventilation strategy.
...from https://news.3m.com/2022-02-24-3M-scientists-This-Corsi-Rosenthal-box-movement-is-legit
January 11, 2021... It's important to note that the effectiveness of portable air filtration devices in reducing the transmission of the SARS-CoV-2 virus hasn't yet been demonstrated. As such, they should not be used alone or as replacement for adequate ventilation, physical distancing and hygienic measures. Whenever possible, consider the use of an alternative space, or preferably gathering outdoors rather than indoors, when interacting with people from outside your household.
Opening windows in winter may not always be comfortable or possible. Doing so for a few minutes at a time during the day can still improve air quality, with minimal impact on the indoor temperature. If occupants will be indoors for longer periods, for example at schools, occupants should have regular outdoor breaks, to allow for ventilation of the room.
Some steam radiators built in older apartment buildings in cities like New York were designed to keep dwellings warm with windows open due to the 1918 pandemic.
...from https://www.snopes.com/fact-check/apartment-radiator-pandemic-spread/
It's impossible to social distance in the car so the next time you're in a car with others, open up the windows at least 3 inches to increase ventilation and lower potential virus levels.
...from (PDF) https://phpa.health.maryland.gov/Documents/Clean%20Your%20Car%20English.pdf
It's important to note, the researchers say, that airflow adjustments are no substitute for mask-wearing by both occupants when inside a car.
...The researchers stress that there's no way to eliminate risk completely -- and, of course, current guidance from the U.S. Centers for Disease Control (CDC) notes that postponing travel and staying home is the best way to protect personal and community health. The goal of the study was simply to study how changes in airflow inside a car may worsen or reduce risk of pathogen transmission.
...from https://www.sciencedaily.com/releases/2020/12/201205143458.htm
Although how we understand transmission occurs has shifted, the ways to prevent infection with this virus have not. All prevention measures that CDC recommends remain effective for these forms of transmission.
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html#
The public may be tired of shifting guidance from the CDC about wearing face masks, but Dr. Anthony Fauci says the latest change wasn't made arbitrarily. Rather, it was forced by the Delta variant. "It isn't that they decided in a vacuum to flip-flop -- the virus changed," he explained in an interview with LX News Now host Eric Alvarez.
Overview
Post-vaccination precautions
When to get tested
Masks
Antigen test flowchart
Quarantine... Short version (YouTube)
Quarantine... Long version
Cleaning
Social distancing is recommended in the Bible.
Vaccines have been around for decades.
The scientific consensus has evolved during the pandemic to support ventilation and masking.
Part of being an expert is knowing what you don't know...
...and knowing what you can't know.
A lot of our early assumptions about the new coronavirus have flip-flopped.
This is normal. That's how science works --it's a process of being less and less wrong over time. COVID-19 is new, so there's lots of uncertainty. And the pandemic's size and scale caught us by surprise. As we learn more, our understanding of the virus continues to change.
The global community is not used to seeing rapidly emerging science and changing policy, and has therefore been desperate for immediate, unambiguous answers. Naturally, intolerance of uncertainty has driven some people to fill this void with deceptive narratives [11, 12].
...from https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-021-06357-4
The CDC did not change their death count.
A doctor talking really fast (TikTok)
underlying medical conditions that increase a person's risk of severe illness from COVID-19
How to fill out a death certificate (YouTube)
The 6 percent number touted by Trump and QAnon comes from a weekly CDC report stating that in 6 percent of the coronavirus mortality cases it counted, COVID-19 was the only condition listed on the death certificate. That observation most likely means that those death certificates were incomplete because the certifiers gave only the underlying cause of death and not the full causal sequence that led to it, Anderson says.
The CDC has identified risky behaviors.
If you engage in risky behavior around an infected person, you're more likely to get sick.
If you follow all the recommended precautions, you won't get sick.
What's the difference between COVID-19 precautions and ordinary safety precautions?
Do you have insurance?
Do you look both ways before crossing the street?
There's no silver bullet.
Multiple imperfect precautions work together. (YouTube)
Controlling the virus requires controlling your behavior. Americans have shown an appalling lack of self-control, so, yes, maybe the governement is trying to control our behavior.
If COVID-19 is a government conspiracy, what should we do?
The CDC recommends specific precautions.
What do the conspiracy theorists suggest we do?
If COVID was intentional/planned/lab leak, does that affect individual citizen's responses?
i.e., we still need to kill it, even if it was intentional/planned/lab leak.
Was COVID engineered intentionally, or are the conspirators just taking advantage of the chaos?
Was death the conspirators' desired result?
Or were the deaths caused by COVID vaccines and COVID restrictions?
If so, was death the goal of the conspirators?
If the conspirators are trying to kill people, why?
Is the goal population control?
Are specific group(s) being targeted?
A better question may be, "Is it safe to go to a restuarant?".
Working in retail is stressful, because people act stupid.
Retail workers don't need anyone else giving them a hard time during a pandemic.
If you can't mask, don't.
Getting emotional about masks may indicate a guilty conscience.
i.e., you're looking for an excuse not to mask.
January 26, 2021... Cochrane (7) and the World Health Organization (8) both point out that, for population health measures, we should not generally expect to be able to find controlled trials, due to logistical and ethical reasons, and should therefore instead seek a wider evidence base. This issue has been identified for studying community use of masks for COVID-19 in particular (9). Therefore, we should not be surprised to find that there is no RCT for the impact of masks on community transmission of any respiratory infection in a pandemic.
October 6, 2020... In hospitals and other health-care facilities, the use of medical-grade masks clearly cuts down transmission of the SARS-CoV-2 virus. But for the variety of masks in use by the public, the data are messy, disparate and often hastily assembled.
...To be clear, the science supports using masks, with recent studies suggesting that they could save lives in different ways: research shows that they cut down the chances of both transmitting and catching the coronavirus, and some studies hint that masks might reduce the severity of infection if people do contract the disease.
...The standard mask for use in health-care settings is the N95 respirator, which is designed to protect the wearer by filtering out 95% of airborne particles that measure 0.3 micrometres (µm) and larger. As the pandemic ramped up, these respirators quickly fell into short supply. That raised the now contentious question: should members of the public bother wearing basic surgical masks or cloth masks? If so, under what conditions? "Those are the things we normally [sort out] in clinical trials," says Kate Grabowski, an infectious-disease epidemiologist at Johns Hopkins School of Medicine in Baltimore, Maryland. "But we just didn't have time for that."
So, scientists have relied on observational and laboratory studies. There is also indirect evidence from other infectious diseases. "If you look at any one paper -- it's not a slam dunk. But, taken all together, I'm convinced that they are working," says Grabowski.
..."You can't do randomized trials for everything -- and you shouldn't." As clinical researchers are sometimes fond of saying, parachutes have never been tested in a randomized controlled trial, either.
...For now, Osterholm, in Minnesota, wears a mask. Yet he laments the "lack of scientific rigour" that has so far been brought to the topic. "We criticize people all the time in the science world for making statements without any data," he says. "We're doing a lot of the same thing here."
Nevertheless, most scientists are confident that they can say something prescriptive about wearing masks. It's not the only solution, says Gandhi, "but I think it is a profoundly important pillar of pandemic control". As Digard puts it: "Masks work, but they are not infallible. And, therefore, keep your distance."
...from https://www.nature.com/articles/d41586-020-02801-8#Fig2
Stuff is restricted in areas where COVID-19 continues to spread.
Why does COVID-19 continue to spread?
There is no easy way out of this, no simple solution that somehow eluded the experts. There is only a miserable tradeoff between economic production and human lives.
After the White House declined to pursue a unified national strategy, governors faced off against lobbyists, health experts and a restless public consumed by misinformation.
...from https://www.nytimes.com/2021/01/17/us/covid-deaths-2020.html#link-4e7d5c01
Effective November 23, 2022, Twitter is no longer enforcing the COVID-19 misleading information policy.
...1. Is the content advancing a claim of fact regarding COVID-19?
...2. Is the claim demonstrably false or misleading?
...3. Would belief in this information, as presented, lead to harm?
...We are most concerned with misleading information that:
· May increase the likelihood of exposure to the virus;
· May have adverse effects on the public health system's capacity to cope with the crisis;
· Could lead to discrimination and avoidance of communities and/or places of business based on their perceived affiliation with protected groups.
...from https://blog.twitter.com/en_us/topics/company/2020/covid-19.html#misleadinginformationupdate
U.S., Food and Drug Administration commissioner Robert Califf told CNN on Saturday evening "almost no one" in the U.S. should be dying from COVID-19, but misinformation was impacting the death toll.
...Califf acknowledged to CNN's Pamela Brow that there's "no way to quantify" his belief that misinformation is the leading cause of death in the U.S., but pointed to "an erosion" of life expectancy" that's on average five years shorter than other high-income countries.
..."Almost no one in this country should be dying from COVID, if we were up to date on our vaccinations and got appropriate anti-viral treatment," Califf said.
Worth noting: Califf, a cardiologist by training, told Brow that what's concerned him for a long time since before the pandemic was the "reduction of life expectancy from common diseases like heart disease," for which a lot of information was available on preventing bad outcomes.
...Califf told a health conference in Austin, Texas, last month he believed misinformation "is now our leading cause of death" in the U.S., per an Association of Health Care Journalists blog.
He pointed to examples including vaccine hesitancy and the popularity of the anti-parasitic ivermectin, which the FDA has urged people not to take as a treatment for the virus, to support his point, according to the AHCJ.
...from https://www.axios.com/2022/05/08/misinformation-us-life-expectancy-drop-fda-chief
A BBC team tracking coronavirus misinformation has found links to assaults, arsons and deaths. And experts say the potential for indirect harm caused by rumours, conspiracy theories and bad health information could be much bigger.
...from https://www.bbc.com/news/stories-52731624#main-heading
At least 800 people may have died around the world because of coronavirus-related misinformation in the first three months of this year, researchers say.
A study published in the American Journal of Tropical Medicine and Hygiene also estimates that about 5,800 people were admitted to hospital as a result of false information on social media.
5G coronavirus conspiracy theory leads to 77 mobile towers burned in UK
In Nigeria, hospital admissions from hydroxychloroquine poisoning provoked Lagos state health officials to warn people against using the drug.
...from https://www.bbc.com/news/stories-52731624#piano-inline3
In Iran, authorities say hundreds have died from alcohol poisoning after viral rumours about its curative effects.
The total was put at 796 by the end of April by Kambiz Soltaninejad, an official from Iran's Legal Medicine Organisation, who said it was the result of "fake news on social media."
The truth behind the number is murky in a country where alcohol is banned in Iran and bootleg moonshine is routinely contaminated.
...from https://www.bbc.com/news/stories-52731624#piano-inline3
During the initial days of the HIV epidemic,47 the rumor that HIV did not exist and its treatment was toxic to humans resulted in people refusing antiretroviral therapies in South Africa. Furthermore, the government promoted traditional medicines that fueled the vertical transmission of HIV in communities and cost >300,000 lives.47
...from https://www.ajtmh.org/view/journals/tpmd/103/4/article-p1621.xml#ref_b46
Brian's may be an extreme case, but with the sheer amount of information circulating - the WHO has called it an "infodemic" - many other people have been misled by what they read online.
They're not killing themselves by taking fake cures. Instead, they're lowering their chances of survival by not thinking coronavirus is real or serious.
...from https://www.bbc.com/news/stories-52731624#piano-inline3
Using a self-administered online survey during the COVID-19 pandemic, the study obtained 483 useable responses and after test, finds that all-inclusive, the propagation of misinformation on social media undermines the COVID-19 individual responses.
...Individual responses, however, regarding the COVID-19 is influenced by the information they received through different media. As mentioned before, the person who died in the USA after consuming chloroquine could be said that he was largely influenced by the message that chloroquine can cure COVID-19.
...from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7373041/#__p1
Mis- and disinformation can be harmful to people's physical and mental health; increase stigmatization; threaten precious health gains; and lead to poor observance of public health measures, thus reducing their effectiveness and endangering countries' ability to stop the pandemic.
Misinformation costs lives. Without the appropriate trust and correct information, diagnostic tests go unused, immunization campaigns (or campaigns to promote effective vaccines) will not meet their targets, and the virus will continue to thrive.
President Trump's lie that "COVID-19 isn't as bad as they say" is why COVID-19 continues to spread--Too many people don't take COVID-19 seriously and aren't vaccinating, social distancing, ventilating and masking. This is why President Trump was kicked off social media.
Conservative hosts Sean Hannity and Tucker Carlson support President Donald Trump, and they are at the helm of the two, most-widely viewed cable news shows in the U.S. But they took different broadcasting paths when the coronavirus first hit the U.S.
The paper notes that Carlson was an outlier on Fox and, as early as Jan. 28, spent a chunk of his show discussing the dangers of a global pandemic. He continued to warn of deadly consequences.
...Meanwhile, Hannity downplayed coronavirus as just the flu and emphasized that Democrats were politicizing the virus to undermine Trump.
...To examine the relationship between viewership of Hannity and Tucker Carlson Tonight and their changes in behavior in response to the coronavirus -- washing hands more often, practicing social distancing and cancelling travel plans -- the authors surveyed 1,045 Fox News viewers aged 55 or older in early April 2020.
The paper says viewership of Hannity relative to Carlson is associated with approximately 30% more COVID-19 cases by March 14, and 21% more COVID-19 deaths by March 28.
The Center for Disease Control has not as yet officially declared exposure to Sean Hannity a public health risk.
"The selective cherry-picked clips of Sean Hannity's coverage used in this study are not only reckless and irresponsible, but down right factually wrong," said a Fox News spokesperson in a statement obtained by Newsweek.
"As this timeline proves, Hannity has covered Covid-19 since the early days of the story." the statement continues. "The 'study' almost completely ignores his coverage and repeated, specific warnings and concerns from January 27-February 26 including an early interview with Dr. Fauci in January. This is a reckless disregard for the truth."
In response, the study's lead author Leonardo Bursztyn noted that their analysis encompasses the entirety of Fox's prime-time coverage through the end of March, including Hannity's interview with Fauci. "There's no 'cherry-picking' possible because our independent MTurk coders read every transcript between late January and late March."
One difference is that SARS-CoV-2 is a "novel" coronavirus, and the scientific consensus changes as we get more data. But the scientific consensus clearly suggests vaccination, social distancing, ventilation and masking. Maybe the difference is just that we don't trust the scientific consensus yet on COVID-19.
https://www.cdc.gov/coronavirus/2019-ncov/your-health/free-masks.html
Because we haven't reached herd immunity, because not enough people are vaccinated or have post-infection immunity.
Can we eradicate COVID-19? (YouTube)
New Covid-19 variants are likely to keep on emerging until the whole world is vaccinated against the virus, experts warn.
Cases tend to rise in areas where:
· Fewer people are vaccinated, which means a large number of people are vulnerable to infection.
· Fewer people are wearing masks.
· More people are gathering indoors to eat, drink, celebrate and socialize without physical distancing.
What makes COVID-19 so resistant to eradication?
A candidate for eradication will typically possess three qualities: an effective intervention that can stop transmission, readily available diagnostic tools that can rapidly detect infection, and a lack of the disease among nonhuman animals. COVID-19 fails on all three counts.
...from https://www.quantamagazine.org/will-we-ever-eradicate-covid-19-20211130/
The initial comment was made by Minnesota State Sen. Scott Jensen, a family physician, who spoke with Fox News host Laura Ingraham on April 8 about the idea that the number of COVID-19 deaths may be inflated.
...In an interview with FactCheck.org, however, Jensen said he did not think that hospitals were intentionally misclassifying cases for financial reasons.
As part of a federal stimulus bill, Medicare is paying hospitals 20% more than standard rates for COVID-19 patients.
Indications are that due to a lack of testing and other factors, the number of coronavirus cases has been undercounted, not padded.
"There's no evidence of hospitals gaming the system to boost payments inappropriately, and there needs to be a documentation of a positive lab test for COVID-19 in the patient's medical record in order to qualify for the 20% payment bump. If they did falsify records to get a pay bump, that would be fraud."
COVID is high-risk.
COVID vaccines are low-risk.
Masks are no-risk for adults.
The virus is encountering a highly vulnerable population of babies and children who were sheltered from common bugs during the pandemic lockdowns.
Immune systems might not be as prepared to fight the virus after more than two years of masking, which offered protection, according to Dr. Elizabeth Mack of Medical University of South Carolina.
“South Carolina is drowning in RSV,” Mack said in a news release. The surge arrived earlier this year than normal, she said.
For babies, their mothers may not have been infected with RSV during pregnancy, which could have given the children some immunity.
Non-pharmaceutical interventions (NPIs) and societal behavioural changes during the COVID-19 pandemic altered not only the spread of SARS-CoV-2, but also the predictable seasonal circulation patterns of many endemic viral illnesses in children.1
...Although many infections and their associated morbidity and mortality were prevented by NPIs, decreased exposure to endemic viruses created an immunity gap—a group of susceptible individuals who avoided infection and therefore lack pathogen-specific immunity to protect against future infection. Decreases in childhood vaccinations with pandemic disruptions to health-care delivery contribute to this immunity gap for vaccine-preventable diseases, such as influenza, measles, and polio.14 The cumulative effect of new susceptible birth cohorts, waning immunity over time with decreased exposures to usual endemic viruses, and lagging vaccination rates in some settings widens this immunity gap and increases the potential for future outbreaks of endemic viruses (figure).
...from https://www.thelancet.com/article/S0140-6736(22)01277-6/fulltext
When you breathe out, the carbon dioxide will go through and round the type of masks most commonly worn, and is unlikely to build up to the extent that it causes health issues.
Surgeons regularly wear much heavier-duty face coverings all day without coming to harm.
In terms of mask-wearing for people with asthma, the CDC explains that in most cases, people with asthma can safely wear masks. And having asthma doesn’t qualify for a mask exemption if and when mask mandates are in place.
Both the Asthma and Allergy Foundation of America (AAFA) and the American Academy of Allergy, Asthma & Immunology (AAAAI) have also lent support to the idea that people with asthma can safely wear facemasks.
The AAFA has stated that in people with well-controlled asthma, wearing a facemask shouldn’t be a safety issue. But people with asthma should take care to manage their condition and take their prescribed medications.
The AAAAI published a 2012 study in The Journal of Allergy and Clinical Immunology that found that oxygen levels didn’t decrease among asthma patients who wore masks. This was the case regardless of the duration of mask-wearing or the type of mask worn.
...from https://www.healthline.com/health/asthma/asthma-mask
Potential Adverse Health Effects of Mask Wearing
Adults
Research supports that under most circumstances, mask wearing has no significant adverse health effects for wearers. Studies of healthy hospital workers, older adults, and adults with chronic obstructive pulmonary disease (COPD) reported no to minimal changes in oxygen or carbon dioxide levels while wearing a cloth or surgical mask either during rest or moderate physical activity.61-65 The safety of mask use during low to moderate levels of exercise has been confirmed in studies of healthy adults and adolescents.64, 66-70 Some,71-74 but not all,67 studies have found that during intense exercise, especially when approaching the aerobic threshold, wearing a mask can increase dyspnea (difficulty breathing), perceived exertion, and claustrophobia, and produce modest negative effects on measured cardiopulmonary parameters. In some people, face masks worn for longer durations might be associated with skin reactions such as acne, itching, dry skin and worsening of existing dermatoses.75-77 Wearing a surgical mask and N95 respirator may have a higher risk of skin reactions compared with a cloth mask.76-78
Children
A study of 60 elementary school children reported no adverse cardiovascular (e.g., heart rate) or pulmonary (e.g., peripheral oxygen saturation) effects among children while wearing a cloth face covering in a classroom for 30 consecutive minutes of instructional time.79 A separate study observed no oxygen desaturation or respiratory distress after 60 minutes of monitoring among children less than 2 years of age when masked during normal play.80 A randomized trial among 40 children aged 3--10 years old scheduled for elective surgery, found that protective surgical face masks could be used safely in the postoperative period.81 In a prospective school-based cohort study of children aged 10--17 years who wore masks for 6--7 hours during the school day, some children self-reported general (4--7%) or situation-specific (2--4%) side-effects such as skin irritation, headache, or difficulty breathing during physical education.82
The potential impact of masks on language and emotional development has been examined in several studies.83-89 Some research suggests children and adults, and especially toddlers (aged 3--5 years) can have difficulty inferring emotion from facial features presented on photographs of persons with their lower facial features covered by a mask.83 However, a study of 7- to 13-year-old children determined the decrement in emotional inference observed when the lower half of a photographed face was covered with a mask was equivalent to that associated with covering the eyes with sunglasses, leading the authors to conclude that in combination with other contextual cues, masks are unlikely to produce serious impairments of children's social interactions.84 A study of 2-year-old children concluded that they were able to recognize familiar words presented without a mask and when hearing words through opaque masks.85 Among children with autism spectrum disorders (ASD), interventions including positive reinforcement and coaching caregivers to teach mask wearing have improved participants' ability to wear a face mask.86-88 These findings suggest that even children who may have difficulty wearing a mask can do so effectively through targeted interventions.
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
A Cornell University study of 38 million articles in English-language media around the world found that US President Donald Trump was the single largest driver of the misinformation.
After the White House declined to pursue a unified national strategy, governors faced off against lobbyists, health experts and a restless public consumed by misinformation.
...from https://www.nytimes.com/2021/01/17/us/covid-deaths-2020.html#link-4e7d5c01
The report noted that the Trump administration recruited Scott Atlas, MD, a radiologist with no background in infectious diseases to serve as an advisor on the response to COVID-19, adding that Atlas received unfettered access to the Trump White House, and became an influential voice pushing for herd immunity policies.
At Atlas's urging, Trump administration officials promoted the herd immunity strategy with "deadly consequences," according to the report.
Specifically, the report stated that Atlas pushed the Trump administration to change CDC guidance to limit the amount of testing conducted in the U.S., and undermined and politicized mask wearing as a mitigation tool, without proposing any alternate measures.
...from https://www.medpagetoday.com/special-reports/features/99362
November 3, 2020... Last month, a coronavirus-crisis sub-committee within the US House of Representatives released a report documenting 47 instances in which government scientists had been sidelined or their recommendations altered. And the report notes that the frequency of meddling has been increasing in the lead-up to the US election.
...from https://www.nature.com/articles/d41586-020-03035-4
The analysis shows that President Trump, Vice President Pence, White House officials, and political appointees at the Department of Health and Human Services (HHS) and other agencies have:
· Pressured health experts to adopt the Administration's talking points, even when they conflict with the science;
· Criticized, sidelined, and fired experts who insisted on sharing accurate scientific information with the public;
· Altered, delayed, and suppressed guidance and scientific reports on testing, protecting children, reopening schools, voting safely, and other topics;
· Authorized questionable virus treatments over the objections of scientists;
· Resisted efforts to ensure the safe development of a vaccine; and
· Diverted $265 million from the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration for an ad campaign to "defeat despair and inspire hope" weeks before Election Day.
On March 13, President Trump declared a national emergency.[468] In mid-March, the Trump administration started to purchase large quantities of medical equipment,[469] and in late March, it invoked the Defense Production Act to direct industries to produce medical equipment.[470]
N95 filtering facepiece respirators can be reused until they are dirty, damaged, or difficult to breathe through. You should inspect your N95 respirator before each time you put it on. If the straps or noseclip are broken, it’s torn, dirty, or otherwise damaged, then you should dispose of it. You should always wash your hands before and after handling your respirator.
The U.S. Centers of Disease Control and Prevention says health care workers can wear an N95 mask up to five times. But experts say how often the average person can safely wear one will vary depending on how it's used.
Using the same mask to run to the grocery store, for example, is very different than wearing it all day at work.
The amount of time a mask is worn is more important than how frequently it's worn, says Richard Flagan, who studies masks and aerosols at the California Institute of Technology.
In general, he recommends limiting the use of an N95 mask to about two or three days.
With every breath you take in an N95, particles accumulate on the mask, Flagan says. That could make it more difficult to breathe if the mask has trapped a lot of particles.
"They are degrading the performance of the mask," Flagan says.
The elastic band on the mask could also get worn out and not fit around your face as snugly. It might also get dirty or wet, especially if you're using it while exercising.
If you notice any of these changes to your mask, it's time to stop using it -- even if you've only used it a few hours. And since N95 masks can't be washed, they should be thrown away once you can no longer use them.
...from https://apnews.com/article/coronavirus-pandemic-science-health-528c5bc4fa4e6d1e73386bcb748176c1
Keep it in a dry, breathable bag (like a paper or mesh fabric bag) to keep it clean between uses.
...from https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/about-face-coverings.html
Our experts recommend storing your mask in a paper bag for 24 to 48 hours in a dry place.
..."It's not the bag that's doing the magic trick, it's actually the process of keeping the mask away from decontaminating someone else or a surface, and also keeping a dry environment in order for the virus to not spread or stay on the mask," explained Dr. Shepherd.
"There have been technologies shown to effectively decontaminate disposable respirators, but those technologies are only available to health care organizations, and are only to be used in crisis situations," Carlson said.
But the latest finding is based on a randomized trial involving nearly 350,000 people across rural Bangladesh.
...The data show that even after 10 washes, surgical masks filter out 76% of small particles capable of airborne transmission of SARS-CoV-2, says Mushfiq Mobarak, an economist at Yale University in New Haven, Connecticut, and a co-author of the study. By contrast, the team found that 3-layered cloth masks had a filtration efficiency of only 37% before washing or use.
A good option: a mask made of two layers of a thick-weave fabric with a built-in pocket where you can place a filter, says May Chu, an epidemiologist at the Colorado School of Public Health who co-authored a paper published on June 2 in NANO Letters on the filtration efficiency of household mask materials.
The best bet for the material to slip in as a filter is polypropylene, which is derived from plastic, says Chu. "If you go to WalMart, you look for Oly-Fun, which is the brand name of that fabric. It's also called spunbond," says Chu, who's a scientific adviser to the World Health Organization and helped craft its recent detailed guidance on cloth masks.
Chu says polypropylene is great as a physical filter but has another benefit: it holds an electrostatic charge -- in other words, it uses the power of static electricity. Think of the static cling that can happen when you rub two pieces of fabric together, says Chu. That's basically what's happening with this fabric: That "cling" effect traps incoming -- and outgoing -- droplets. "That's what you want -- the cling is what's important," Chu says.
And unlike other materials, polypropylene keeps its electrostatic charge in the humidity created when you breathe out, says Yi Cui, a professor of materials science and engineering at Stanford University who co-authored the Nano Letters study with Chu.
Cui and Chu note that polypropylene will lose its electrostatic charge when you wash it, but you can recharge it by ironing it or by rubbing it with a plastic glove for around 20 seconds. Once you've got static cling, ka-ching -- you're back in business.
...Early in the pandemic, the Centers for Disease Control and Prevention (CDC) recommended that anyone symptomatic for suspected coronavirus disease 2019 (COVID-19) should wear a face covering during transport to medical care and prior to isolation to reduce the spread of respiratory droplets. After emerging data documented transmission of SARS-CoV-2 from persons without symptoms, the recommendation was expanded to the general community, with an emphasis on cloth face coverings that could be made more widely available in the community than surgical masks and to preserve personal protective equipment such as N95 respirators to the highest-risk exposures in health care settings. Now, there is ample evidence that persons without symptoms spread infection and may be the critical driver needed to maintain epidemic momentum.[94]
...from https://zeynep.substack.com/p/small-data-big-implications
Close Contact through proximity and duration of exposure: Someone who was less than 6 feet away from an infected person (laboratory-confirmed or a clinical diagnosis) for a cumulative total of 15 minutes or more over a 24-hour period (for example, three individual 5-minute exposures for a total of 15 minutes). An infected person can spread SARS-CoV-2 starting 2 days before they have any symptoms (or, for asymptomatic people, 2 days before the positive specimen collection date).
...from https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tracing-plan/appendix.html
"One thing that might be different with the variants is that people could be shedding more virus into the air.... You're exposed to more virus, so your chances of infection are higher," she said. "Another thing that might be different is that the infectious dose could be lower."
Marr said there seems to be a "significant change" with masks against Omicron and its subvariants, meaning a cloth mask that may have been somewhat protective before is no longer sufficient and that higher-quality masks may be necessary.
...from https://www.cbc.ca/news/health/covid-19-risk-canada-omicron-sixth-wave-1.6420210
Mask math (YouTube)
More masks = less risk
There's no silver bullet.
Multiple imperfect precautions work together. (YouTube)
RSV surged when we stopped masking.
Observational and epidemiological studies on masks
Limitations of mask studies
The relationship between source control and wearer protection is likely complementary and possibly synergistic, so that individual benefit increases with increasing community mask use.
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
Start with a surgical mask closest to your face, says Marr, and then add a cloth one on top. You want a surgical mask made out of a nonwoven material called polypropylene, because that material holds an electrostatic charge that allows it to trap particles. (Some surgical masks are made of paper.)
The downside of surgical masks is that many of them fit loosely -- and a mask's ability to filter out particles depends partly on how well it seals to your face. By layering a cloth mask on top, you can achieve a tighter fit while also adding an extra layer of filtration, says Marr, who co-wrote a recent commentary recommending double-masking.
Correct and consistent mask use is a critical step that people can take to protect themselves and others from COVID-19. However, the type of masks used, and whether or not they are used consistently and correctly varies throughout the general population. Therefore, mask use is not considered when determining COVID-19 exposure and the definition of a close contact during case investigation and contact tracing, regardless of whether the person diagnosed with and/or the person exposed to COVID-19 was wearing a mask. (Note: Exposure risk in the healthcare setting is determined separately and outlined in CDC guidance).
How long are you safe with different kinds of masks?
Different materials... Filtration efficiency
Different materials... Protection efficiency... Inward & outward
Different materials... How many particles get through?
...from https://www.medrxiv.org/content/10.1101/2020.11.18.20233353v1.full
But the latest finding is based on a randomized trial involving nearly 350,000 people across rural Bangladesh.
...The study linked surgical masks with an 11% drop in risk, compared with a 5% drop for cloth.
There have been some studies of cloth masks, which have been found to be less protective than surgical masks in most, but not all, cases.
...from https://www.medrxiv.org/content/10.1101/2020.11.18.20233353v1.full-text
Although cloth masks may appear to be more substantial than the paper surgical mask option, surgical masks as well as KN95 and N95 masks are infused with an electrostatic charge that helps filter out particles.
Multi-layer cloth masks can both block 50-70% of these fine droplets and particles3, 14 and limit the forward spread of those that are not captured.5, 6, 15, 16 Upwards of 80% blockage has been achieved in human experiments,4 with cloth masks in some studies performing on par with surgical masks as barriers for source control.3, 9, 14, 17
...from https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
According to fit tests on 21 adults in the same study, homemade, 100% cotton masks provided median inward filtration efficiencies of 50%, compared to 80% for surgical masks.
...from https://www.medrxiv.org/content/10.1101/2020.11.18.20233353v1.full
Homemade masks made from tea cloths and worn by volunteers had a median inward filtration efficiency of 60%, compared to 76% for a surgical mask (van der Sande, Teunis and Sabel 2008).
...from https://www.medrxiv.org/content/10.1101/2020.11.18.20233353v1.full
"a surgical mask is better than a cloth mask, a tight-fitting surgical mask is better than a loose-fitting mask, and an N95 is better than a surgical mask."
...from https://www.vox.com/22220301/covid-spread-new-strain-variants-safe-grocery-store-n95-masks-vaccine
The best homemade cloth masks actually achieved better filtration (79 percent) than surgical masks (62 percent to 65 percent) in a peer-reviewed study at the Wake Forest Institute of Regenerative Medicine published in April. In the study, the best cloth masks were made of heavyweight quilter's cotton with a thread count of 180 or more. Masks with even thicker thread, tightly woven like a batik, and double-layer masks with a basic cotton outer and flannel inner also proved effective.
...from https://hartfordhealthcare.org/about-us/news-press/news-detail?articleId=26004&publicid=745
An N95 must be able to protect an individual worker in high-risk situations. A critical component of its efficacy is the fit test to ensure that the respirator seals completely to the face with no leaks. On the other hand, the overall goal of wearing cloth masks during the COVID-19 pandemic is to reduce community transmission.
...from https://www.medrxiv.org/content/10.1101/2020.11.18.20233353v1.full
The filtration, effectiveness, fit, and performance of cloth masks are inferior to those of medical masks and respirators. Cloth mask use should not be mandated for healthcare workers, who should as a priority be provided proper respiratory protection. Cloth masks are a more suitable option for community use when medical masks are unavailable. Protection provided by cloth masks may be improved by selecting appropriate material, increasing the number of mask layers, and using those with a design that provides filtration and fit. Cloth masks should be washed daily and after high-exposure use by using soap and water or other appropriate methods.
...from https://wwwnc.cdc.gov/eid/article/26/10/20-0948_article
For any style [of beard], hair should not cross under the respirator sealing surface.
Gaps can be caused by choosing the wrong size or type of mask and when a mask is worn with facial hair.
...from https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/types-of-masks.html
How beard length affects different types of masks
Though variable, N95 respirators offer the best respiratory protection for bearded men. While KF94 and KN95 FFE is compromised considerably by increasing beard length, they proved better options than procedure and cotton face masks. A simple exercise band improves FFE for face masks commonly used by bearded men during the COVID-19 pandemic.
Or click "DOWNLOAD" at the top right of the Axios/Ipsos poll to download the latest PDF.
Then search for "mask" in the PDF.
All results show percentages among all respondents, unless otherwise labeled.
...from https://www.ipsos.com/sites/default/files/ct/news/documents/2022-08/Wave%2069%20Topline_0.pdf
Health Equity Considerations and Racial and Ethnic Minority Groups
Of course, not everyone has the privilege of social distancing. From the United Kingdom to Sweden to Canada, we have evidence that the virus preys on people employed in "essential service" jobs (bus drivers, nurses, factory workers), which don't allow for telecommuting or paid sick leave; people in low-income neighborhoods; and people in "congregate housing" like shelters, prisons, and retirement homes.
People of color tend to be overrepresented in these groups -- but there's no biological reason they're more likely to get sick and die from the virus. Simply put: They tend to work jobs that take them outside the home and into close contact with other people, live in crowded environments ideal for coronavirus contagion, or both.
...from https://www.vox.com/22220301/covid-spread-new-strain-variants-safe-grocery-store-n95-masks-vaccine
White Americans are far more likely to outlive Black Americans. They live longer for a whole myriad of reasons, like differences in access to care, trauma, stress, etc. This is important because age is the strongest risk factor, by far, for dying of COVID.
If we account for age, we see a very different story. Below is data from a database called CDC WONDER. The 2022 death data is provisional (which means it’s not the official count because death certificates take a long time to process), but it’s the best we have. I pulled all COVID deaths for 2022 and organized by race. Before adjusting for age, White Americans account for 43 per 100,000 in 2022 compared to, for example, Black Americans, who account for 37 per 100,000. After we adjust for age, the story changes: Whites account for 31 per 100,000 while Blacks account for 40 per 100,000. A complete switch.
...from https://yourlocalepidemiologist.substack.com/p/the-morning-today-iswrong
But what started as a health emergency concentrated in travelers, urban minority communities, and other crowded places (such as nursing homes and prisons) fanned out into rural areas of the country, leading to a surge in deaths among white people, too.
...By October, some of the most sparsely populated areas of the country -- Wyoming, the Dakotas, Nebraska -- were grappling with America's worst outbreaks. The relative share of deaths among white people started rising.
"The politics of 2020 led governors in [these] parts of the country to be less aggressive in dealing with the virus or actively discourage public health safeguards," Woolf said.
At the same time, more states adopted face-mask orders and other safety measures. Mask mandates helped bring case numbers down, and may have saved the lives of some essential workers.
The result: In August, Black people died at 2.5 times the rate of white people. By November, the rate was 2.2. In early February, it was 1.5.
...To prevent more needless suffering, we need to heed the lesson of the Covid-19 deaths in 2020: "The health haves cannot keep ignoring the health have-nots," Sandro Galea said. "Because everyone is susceptible to Covid, the fact [that] higher-risk groups exist makes everybody vulnerable."
...from https://www.vox.com/22252693/covid-19-deaths-us-who-died#t3SKUw
Do you open your Bible?
Or do you pray?
Or do you go to the doctor?
The Bible gives general principles, but it doesn't say how many people died in 2020 and 2021 or how many unvaccinated vs vaccinated people died of COVID or how natural immunity compares to vaccine-induced immunity.
Therefore I shall ask God mercifully to protect us. Then I shall fumigate, help purify the air, administer medicine, and take it. I shall avoid places and persons where my presence is not needed in order not to become contaminated and thus perchance infect and pollute others, and so cause their death as a result of my negligence.
Modern scientists rely on the regularities of nature that are a product of God's wisdom and faithfulness. But for many, a distortion enters in, because they think that the regularities or "laws of nature" are ultimately impersonal. If they are impersonal, they are basically like a mechanism, for which there can be no exceptions. So before even reading the Bible or listening to the evidence, they think they "know" that there can be no exceptions and no miracles.
This antibiblical view of the world has consequences. Science can still succeed in many ways, because the distorted conception is close enough to the reality to enable advances. At the same time, it is bound to come into conflict with the Bible when it comes to reconstructions of the past.
...from https://www.thegospelcoalition.org/essay/the-bible-and-science/
Scientists are specialists. I don't think evolutionary biologists are making COVID-19 recommendations. I don't think virologists, epidemiologists and immunologists are pushing evolution.
My speciality is the Bible. I don't know as much about evolution as an evolutionary biologist does. Does evolution address origins? Does the Bible say how God created the universe? Could God have used evolution in the creation process? There may be some answers here and here... I haven't read those two pages yet, but I have found Wikipedia invaluable for controversial subjects.
I think it's important to know what you don't know. We rely on specialists when our knowledge is limited. If we can't read Greek or Hebrew, we use English Bible translations.
The Bible doesn't say how to treat COVID-19. It provides general principles, but I think COVID-19 needs to be scientifically discerned, similar to Bible translations.
Can a scientist who believes in evolution do good COVID-19 science? Does your religion affect the quality of your work? Can unbelievers do worthwhile work?
Science isn't biased.
Is science opposed to faith?
At this point, most people realize that the debate is not about operation science, which is based in the present. The debate is about origin science and conflicting assumptions, or beliefs, about the past.
...from https://answersingenesis.org/what-is-science/science-or-the-bible/
Jesus' forgiveness is not a license to sin.
God's protection is not a Get-out-of-jail-free card.
Should we cower in fear before a virus? Certainly not.
Should we obey every last whim and dictate of the government, even when local administrations are guilty of dangerous overreach? Absolutely not, as the Department of Justice recently affirmed as well.
But we should not put the Lord to a test. In other words, we should not willingly and needlessly put ourselves in harm's way and expect a miracle from Him.
...from https://www.christianpost.com/voices/do-not-put-the-lord-your-god-to-the-test.html
Therefore I shall ask God mercifully to protect us. Then I shall fumigate, help purify the air, administer medicine, and take it. I shall avoid places and persons where my presence is not needed in order not to become contaminated and thus perchance infect and pollute others, and so cause their death as a result of my negligence. If God should wish to take me, he will surely find me and I have done what he has expected of me and so I am not responsible for either my own death or the death of others. If my neighbor needs me, however, I shall not avoid place or person but will go freely, as stated above. See, this is such a God-fearing faith because it is neither brash nor foolhardy and does not tempt God.
25"For this reason I say to you, do not be worried about your life, as to what you will eat or what you will drink; nor for your body, as to what you will put on. Is not life more than food, and the body more than clothing? 26"Look at the birds of the air, that they do not sow, nor reap nor gather into barns, and yet your heavenly Father feeds them. Are you not worth much more than they? 27"And who of you by being worried can add a single hour to his life? 28"And why are you worried about clothing? Observe how the lilies of the field grow; they do not toil nor do they spin, 29yet I say to you that not even Solomon in all his glory clothed himself like one of these. 30"But if God so clothes the grass of the field, which is alive today and tomorrow is thrown into the furnace, will He not much more clothe you? You of little faith! 31"Do not worry then, saying, 'What will we eat?' or 'What will we drink?' or 'What will we wear for clothing?' 32"For the Gentiles eagerly seek all these things; for your heavenly Father knows that you need all these things. 33"But seek first His kingdom and His righteousness, and all these things will be added to you.
34"So do not worry about tomorrow; for tomorrow will care for itself. Each day has enough trouble of its own.
(Matthew 6:25-34, NASB95)
We can't prolong our life by worrying.
In 2020, life expectancy at birth in the U.S. dropped by 1.8 years, the biggest yearly decrease since World War II.
...from https://www.medpagetoday.com/opinion/second-opinions/100388
Life expectancy at birth decreased 0.6 year from 77.0 in 2020 to 76.4 in 2021, largely because of increases in mortality due to COVID-19, unintentional injuries, chronic liver disease and cirrhosis, suicide, and homicide.
...from https://www.cdc.gov/nchs/products/databriefs/db456.htm
But we can shorten our life by taking unnecessary risks.
If you engage in risky behaviors around an infected person, you're more likely to get infected.
Don't come to church if you have cold symptoms.
Wear a mask to protect others, especially if you're not vaccinated.
Don't shake hands or kiss.
Bring a jacket or sweater, because windows may be open.
Vaccines reduce infections:
Provide masks?
Can our HVAC increase outside air exchange?
No multiple services on the same day?
Cancel services?
Cleaning between services isn't necessary.
Similarly, Loudon and Roberts investigated the role of singing in the spread of tuberculosis and showed that the percentage of airborne droplet nuclei generated by singing is 6 times more than that emitted during normal talking and approximately equivalent to that released by coughing27. More recent work using advanced particle characterization techniques have yielded similar results21,28,29,30



mark@chiptape.com
.png?sfvrsn=a8b9e94_4){kind=link}
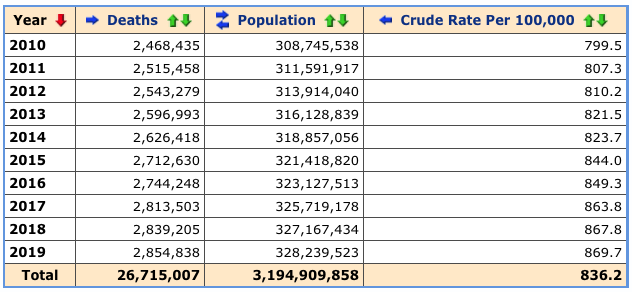{kind=link}
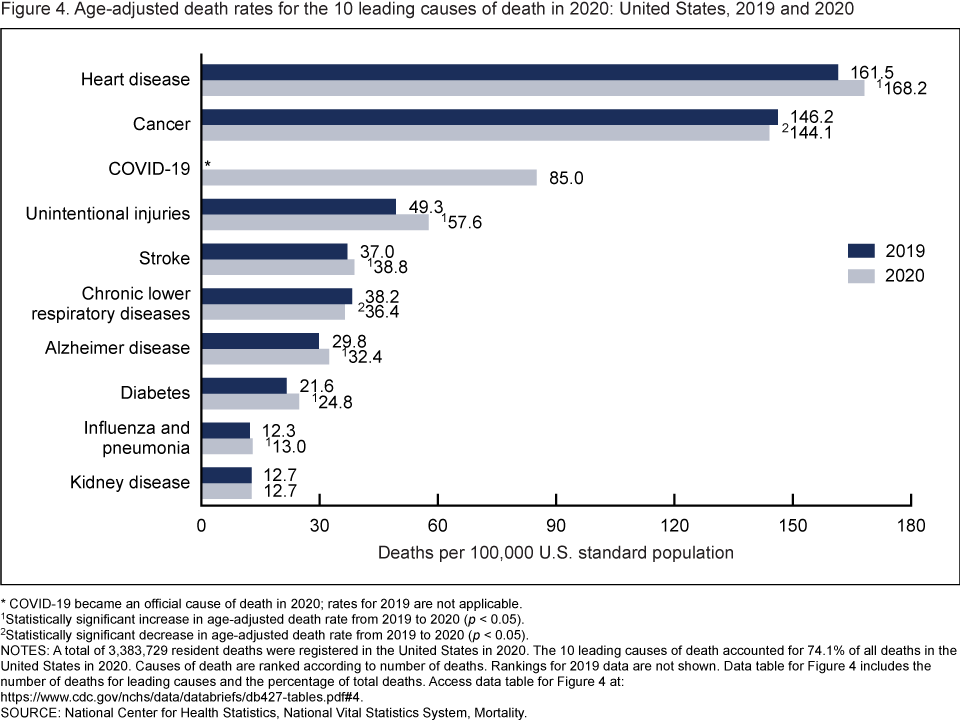{kind=link}
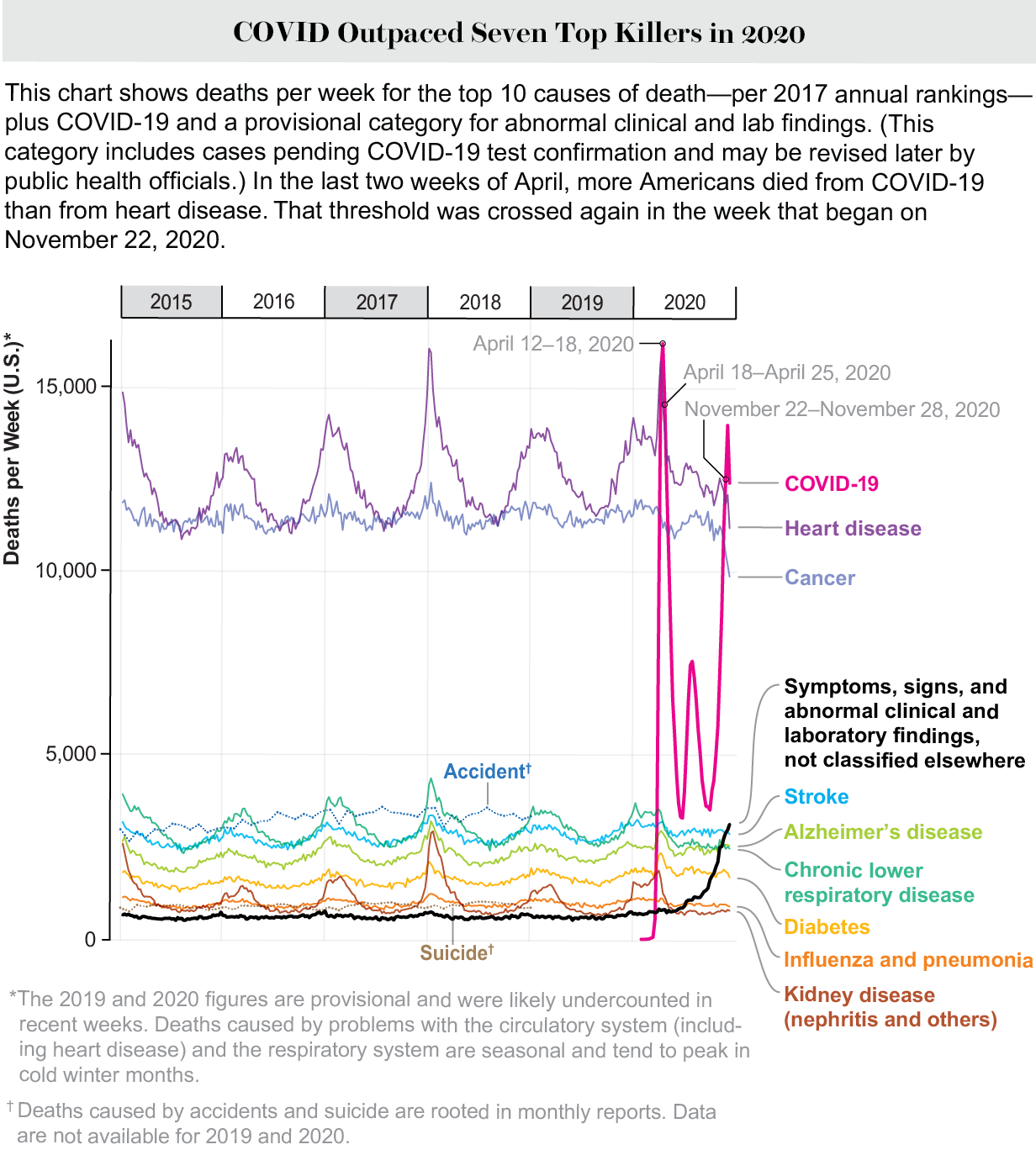{kind=link}
{kind=link}
{kind=link}
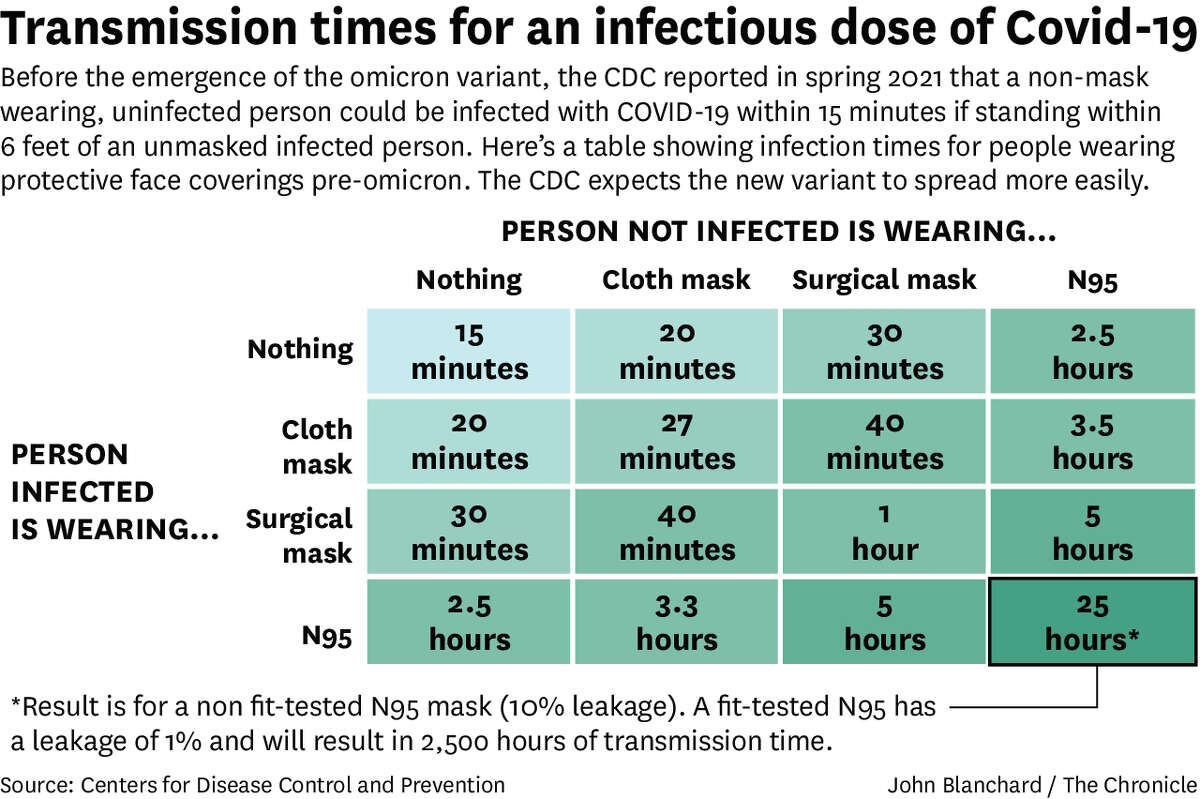{kind=link}
{kind=link}
{kind=link}
{kind=link}